Diagnosis: Grade IV hepatic injury with pseudoaneurysm and active extravasation
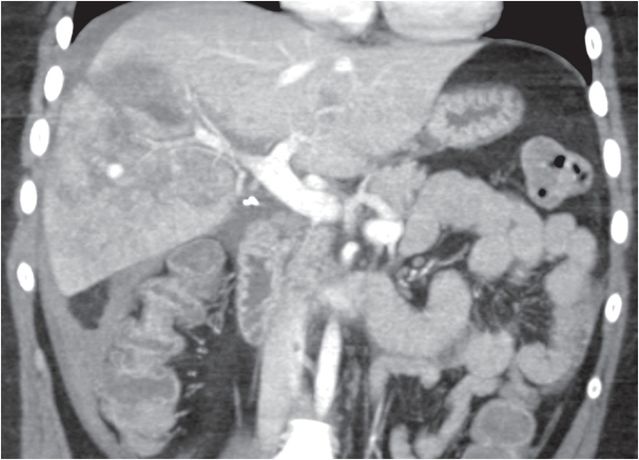
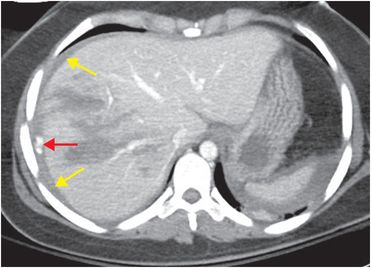
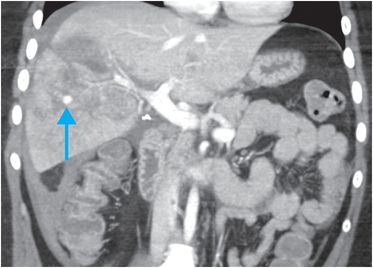
Axial and coronal contrast-enhanced CT demonstrates multiple linear, low-attenuation hepatic lacerations involving the right hepatic lobe, extending from the surface of the liver into the parenchyma. There is a low-attenuation subcapsular hematoma (yellow arrows) containing a focus of active extravasation of intravenous contrast (red arrow) adjacent to the liver capsule. An additional focus of extravascular contrast pooling within the hepatic parenchyma (blue arrow) represents a traumatic pseudoaneurysm.
Discussion
Overview of liver trauma
The liver is the second most commonly injured abdominal organ in trauma after the spleen. Hepatic injury may occur with blunt (most common) or penetrating trauma, including iatrogenic trauma.
The right hepatic lobe is more commonly injured than the left. When the left hepatic lobe is injured, it is important to assess for concurrent bowel and pancreatic injury.
Grading of liver trauma
Hepatic injury is graded according to the American Association for the Surgery of Trauma (AAST) classification system.
Grades I–III injuries are classified based on the presence, size, and extent of laceration (linear or branching hypoattenuating areas within the hepatic parenchyma, usually extending from the capsular surface), subcapsular hematoma (hypoattenuating, lenticular collection of blood between the liver parenchyma and capsule), and intraparenchymal hematoma (irregular-shaped hypoattenuating collection within the hepatic parenchyma). Additionally, the presence of active hemorrhage (focus of extravasated contrast) indicates that the injury is at least grade III, and is a strong predictor of failure of conservative management.
In hemodynamically stable patients, contrast-enhanced CT of the abdomen and pelvis is the imaging modality of choice. CT allows rapid assessment of extent and severity of hepatic injury, particularly active extravasation and vascular injury, as in the index case, in addition to injuries involving other organs. Unstable patients usually undergo emergent exploratory laparotomy without imaging.
| Grade | ||
|---|---|---|
| I | Subcapsular hematoma | <10% of surface area |
| Laceration | <1 cm in depth | |
| II | Subcapsular hematoma | 10–50% of surface area |
| Intraparenchymal hematoma | <10 cm diameter | |
| Laceration | 1–3 cm in depth | |
| III | Subcapsular hematoma | >50% of surface area (or expanding in size) or actively bleeding |
| Intraparenchymal hematoma | >10 cm diameter or expanding or actively bleeding | |
| Laceration | >3 cm in depth | |
| IV | Intraparenchymal hematoma | ruptured with active bleeding |
| Laceration | parenchymal disruption involving 25–75% of the hepatic lobes or 1–3 Couinaud segments within one lobe | |
| V | Laceration | parenchymal disruption involving >75% of the hepatic lobes or >3 Couinaud segments within one lobe |
| Vascular | venous injuries involving the IVC or major hepatic veins | |
| VI | Vascular | hepatic avulsion |
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


