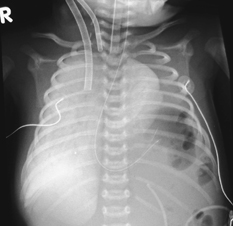
CASE 63 This 3-day-old neonate with a known prenatal ultrasound diagnosis was intubated and ventilated following delivery. Extracorporeal membranous oxygenation (ECMO) was then instigated. Figure 63A Chest radiograph (Fig. 63A) demonstrates multiple rounded lucencies within the left hemithorax with mediastinal shift to the right. The tips of the arteriovenous ECMO catheters are positioned in the right atrium (radiodense dot distal to the opaque linear portion of the venous catheter) and in the origin of the right common carotid artery or aortic arch (there is a small radiolucent portion beyond the apparent radiodense tip). Left congenital diaphragmatic hernia (CDH) CDH occurs with an incidence of 1 to 2 in 3000 live births. The vast majority occur posterolaterally through the foramen of Bochdalek, with 75% of cases on the left. Herniation of abdominal contents into the thoracic cavity through a defect in the diaphragm results in varying degrees of pulmonary hypoplasia. Most Bochdalek hernias are detected on prenatal ultrasound or present with respiratory distress and difficulty in resuscitation at birth. The abdomen is scaphoid with absent breath sounds in the affected hemithorax and displacement of the apex beat. Smaller lesions may present in later childhood with recurrent respiratory infections, constipation, or symptoms of GI obstruction. Strangulation or volvulus is an unusual but potentially fatal presentation. There is an increased incidence of delayed right-sided Bochdalek hernia following neonatal streptococcal pneumonia, the etiology of which is not fully understood. Further cases are associated with trauma, either acutely or with a delayed presentation. Small lesions may be asymptomatic, an increasing number of which are now being recognized on CT as an incidental finding. Morgagni hernias generally present later in childhood or in adult life, often as an asymptomatic finding but sometimes associated with abdominal pain, vomiting, or chest pain. Rare neonatal cases present with respiratory distress. Figure 63B
Clinical Presentation

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Pathology/Embryology
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


