Diagnosis: Distal right ureteral injury
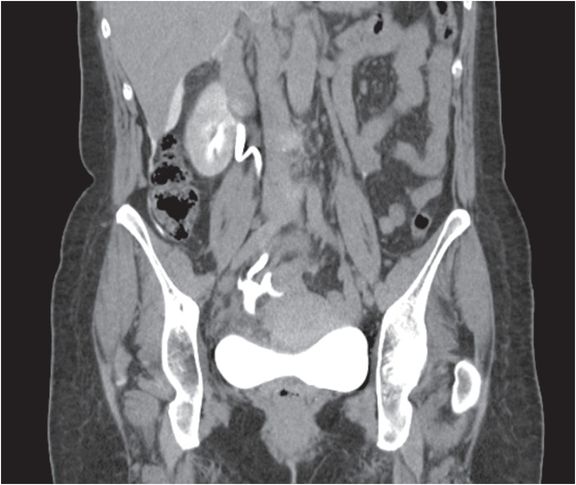
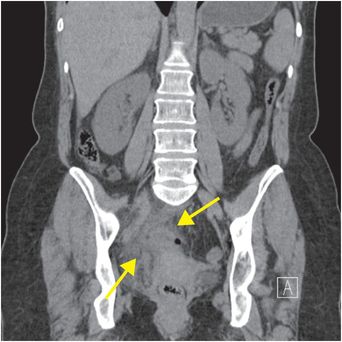
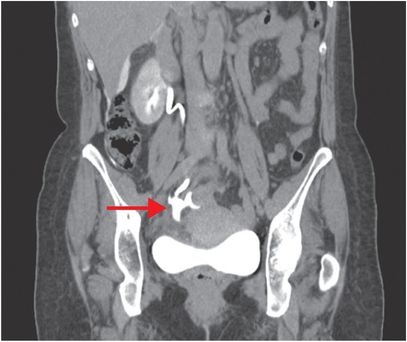
Unenhanced coronal CT of the abdomen and pelvis (left image) demonstrates fat stranding and fluid in the right hemipelvis, in the vicinity of the right distal ureter (yellow arrows). Delayed coronal CT (right image) obtained 15 minutes after administration of IV contrast demonstrates opacification of the right renal collecting system and ureter, with an irregular collection of extraluminal contrast denoting injury of the distal right ureter (red arrow).
Discussion
Ureteral injury may result from blunt, penetrating, or iatrogenic trauma. The most common cause of ureteral injury is iatrogenic trauma (80–90%) incurred with gynecologic, urinary tract, retroperitoneal, and pelvic surgeries.
Delayed diagnosis is common due to the nonspecific clinical presentation.
Penetrating injury may result in direct transection of the ureter and is usually accompanied by other intra-abdominal injuries. Blunt trauma from deceleration mechanisms may cause avulsion at the ureteropelvic junction.
The AAST classification of ureteral injury is as follows:
Grade I – Hematoma; contusion or hematoma without devascularization
Grade II – Laceration; <50% transection
Grade III – Laceration; >/= 50% transection
Grade IV – Laceration; complete transection with <2 cm devascularization
Grade V – Laceration; avulsion with >2 cm devascularization
*Advance one grade for bilateral injury, grades I–III.
Contrast-enhanced CT of the abdomen and pelvis must include a delayed phase (10–20 minutes after contrast administration) to adequately assess the renal collecting systems and ureters. A less frequently used alternative is fluoroscopic retrograde pyelography. Scintigraphy may be used in patients who are unable to receive iodinated contrast (e.g., due to renal failure or contrast allergy).
Treatment varies based on severity. A ureteral stent may be left in place for 4–8 weeks to promote uroepithelial healing. Associated urinomas may be drained percutaneously. Early identification leads to improved clinical outcomes. When diagnosis is delayed, ureteral strictures may form, necessitating balloon dilatation. Surgery is typically reserved for cases of complete ureteral transection or strictures that do not improve with balloon dilatation.
Clinical synopsis
The patient was admitted to the hospital for a short period of time, and a ureteral stent was left in place for approximately 8 weeks. Upon removal of the ureteral stent, repeat imaging showed no extraluminal contrast or urinary obstruction, indicating complete ureteral healing.
Self-assessment
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


