Diagnosis: Anterior posterior compression (APC) type 2 pelvic ring injury
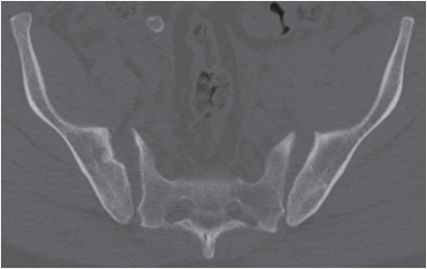
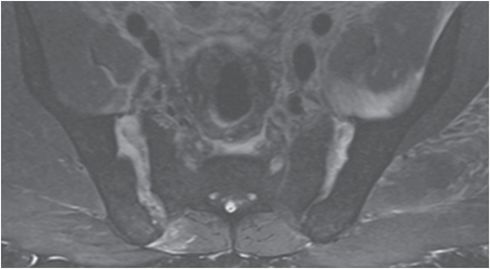
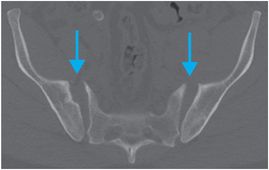
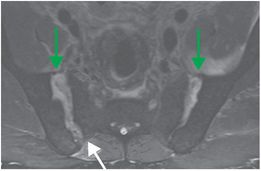
AP radiograph of the pelvis (left image) demonstrates a displaced fracture through the roof of the left acetabulum (yellow arrow) with posterior dislocation of the hip. There is marked pubic symphyseal diastasis (red arrow) of greater than 2.5 cm, with apparent broadening of the right iliac wing. Axial CT (middle image) demonstrates widening of the anterior aspects of the right greater than left anterior sacroiliac (SI) joints (blue arrows). Axial proton density MRI with fat suppression (right image) shows disruption of both anterior SI ligaments (green arrows) and confirms widening of the anterior SI joint spaces. Thickening and edema of the right posterior SI ligament (white arrow) suggests sprain or partial tear, in contrast to the normal left posterior SI ligament. This is an anterior posterior compression (APC) type 2 injury given the pubic symphysis diastasis of > 2.5 cm and widening of the anterior sacroiliac joints.

Discussion
The pelvis is a ring structure composed of the sacrum and paired innominate bones, which are joined anteriorly at the pubic symphysis (anterior arch) and posteriorly at the sacrum via the SI joints (posterior arch).
The pubic symphysis, which is the weakest portion of the pelvic ring, is stabilized by the superior and inferior pubic ligaments.
The posterior arch is stabilized by the anterior and posterior interosseous SI ligaments. The anterior SI ligaments resist internal rotation, while the stronger posterior SI ligaments resist external rotation and vertical displacement.
Pelvic ring injuries usually occur in high-impact trauma due to transfer of a large amount of kinetic energy: motor vehicle accidents, falls from height, and crush injuries are the most common etiologies.
Associated injuries may be caused by primary impact, osseous fragments, or secondary to shear forces, and include vascular disruption, hemorrhage, urogenital injury, lumbosacral plexus disruption, and long bone fracture.
As in other complex fracture scenarios, understanding the mechanism of injury can refine the search for additional injuries. Analogous to injury of other ring structures such as the mandible, fracture in one portion of the pelvic ring should prompt a search for fracture or ligamentous injury in a second location.
In the setting of trauma, the pelvic ring can be radiographically evaluated using a standard AP view, pelvic inlet and outlet (Ferguson) views, and in some cases, with CT or MRI.
The inlet view is useful for characterizing anterior–posterior fracture displacement, while the outlet view is useful for identifying vertical displacement.
CT or CT cystography is useful for evaluation of the pelvic organs in severe trauma, and for further evaluation of pelvic fractures identified by radiography.
In the emergency setting, pelvic MRI image can be abbreviated to coronal STIR and coronal T1-weighted imaging. These limited sequences have high sensitivity for fracture, avascular necrosis of femoral head, and soft tissue injury. MRI should be considered when radiographically occult or insufficiency-type fractures are suspected.
The Young and Burgess classification, based on the force vector, classifies pelvic ring injuries as lateral compression (50–70%), APC (20–30%), vertical shear (14%), or combined mechanism injuries.
APC injury results from head-on motor vehicle collisions where the force vector is directed in the anterior to posterior direction in the sagittal plane. This force causes external rotation at one or both SI joints, resulting in open-book type injury. Injury may be unilateral or bilateral. An associated finding is broadening of the iliac wing on the AP view. A summary of the features of APC injuries by grade is presented in the table below.
| APC injury type | Pubic symphysis diastasis | Effect on SI joints | Rotational stability | Vertical stability |
|---|---|---|---|---|
| APC 1 | < 2.5 cm | None | Preserved | Preserved |
| APC 2 | > 2.5 cm | Anterior joint widening | Compromised | Preserved |
| APC 3 | Complete disruption | Complete disruption of SI ligaments with dissociation of the iliac wing and sacrum | Compromised | Compromised |
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 51 90-year-old male with elevated blood pressure and change in mental status. No history of trauma
51 90-year-old male with elevated blood pressure and change in mental status. No history of trauma
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


