CASE 74 Antenatal ultrasonography shows a large bladder and bilateral hydro-ureteronephrosis in a boy. Figure 74A Figure 74B Images from voiding cystourethrography (VCUG) with a urethral catheter in place (Fig. 74A), and with the catheter removed (Fig. 74B), show a dilated posterior urethra with a sudden change in the caliber at the prostatic-penile junction and a narrow stream of contrast through the anterior urethra. There is bladder irregularity posteriorly, with reflux of contrast into a tortuous dilated left ureter, and into a hydronephrotic kidney with additional intrarenal reflux (international grade 5). Posterior urethral valves (PUVs) with unilateral vesicoureteral reflux PUVs affect boys only, with an incidence of approximately 1 in 10,000. It is the commonest obstructive uropathy in male children. Typical prenatal ultrasonographic findings include bilateral hydronephrosis with a large bladder with or without progressive oligohydramnios. Many cases are now suspected from prenatal ultrasonography and are examined by VCUG soon after birth. PUV have been traditionally classified into three or four types, but in reality only two types are seen. Type 1 is the most common, seen in approximately 95% of cases, where two folds at the verumontanum have a ventral slitlike orifice. Type 3 has a pinpoint orifice that results in forward ballooning of the valve during VCUG, giving a so-called wind-in-the-sail appearance. In actual practice, it is usually impossible to tell type 1 from type 3 valves on VCUG. Type 3 valves have a higher association with renal dysplasia. Vesicoureteral reflux is commonly associated with PUV. Occasionally, bladder hypertrophy is such that reflux no longer occurs, but the ureters remain dilated.
Clinical Presentation

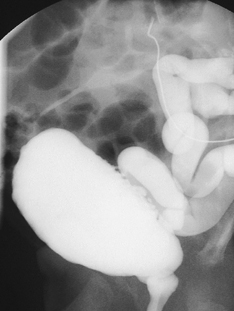
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


