Diagnosis: Anterior shoulder dislocation
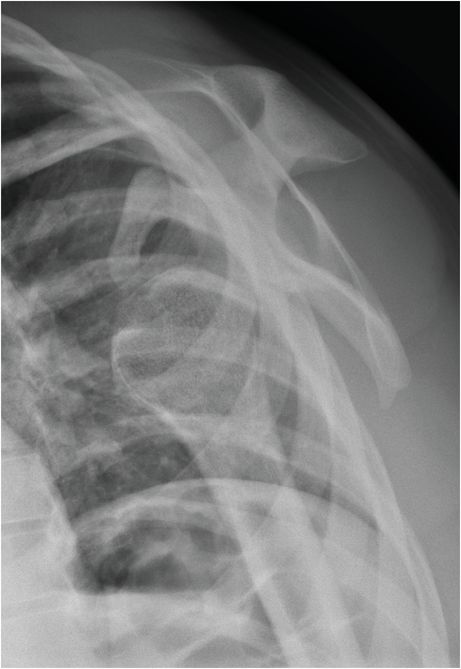
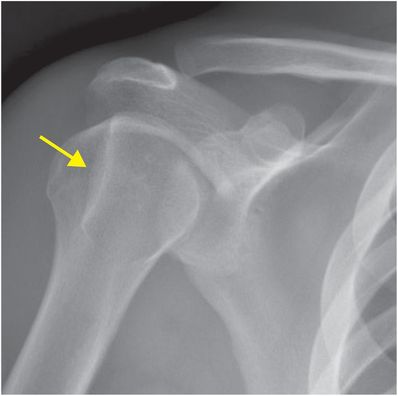
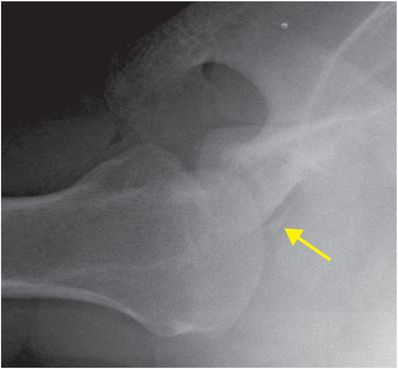
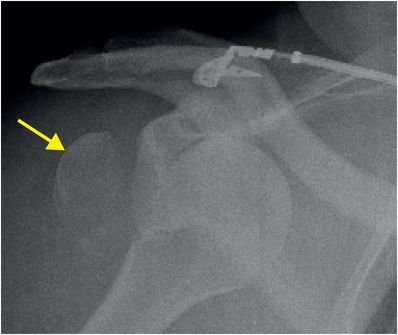
AP radiograph of the shoulder (left image) demonstrates an anterior subcoracoid shoulder dislocation with the humeral head (yellow arrow) inferiorly displaced relative to the glenoid. Scapular-Y radiograph of the shoulder confirms that the humeral head (yellow arrow) is dislocated anterior to the glenoid and inferior to the coracoid process (red arrow).
Discussion
Overview of glenohumeral dislocation
Glenohumeral dislocation is defined as complete loss of glenohumeral articulation. In contrast, subluxation is characterized by partial articulation of the humeral head with the glenoid. Shoulder dislocation is classified based on direction, humeral head location, and presence of associated injuries.
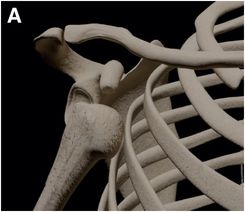
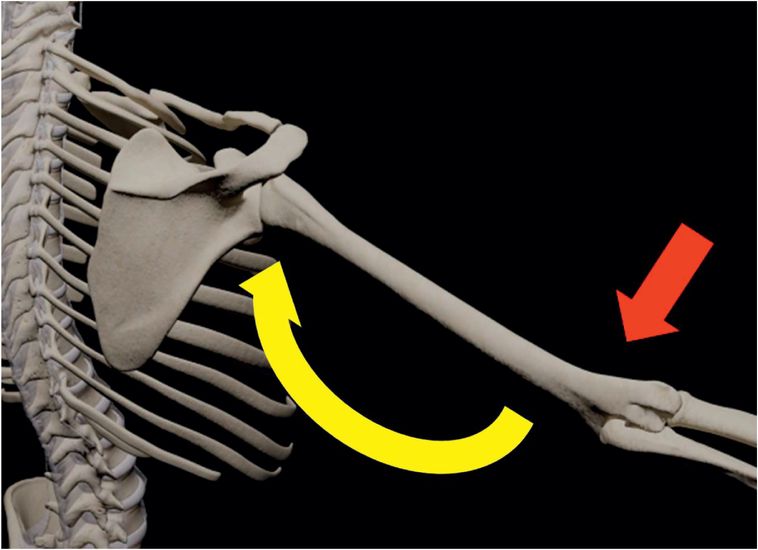
The vast majority of shoulder dislocations are anterior in direction (~95%), and are further subclassified as subcoracoid (A), subglenoid (B), or subclavicular (C) based on resting pre-reduction position of the humeral head.
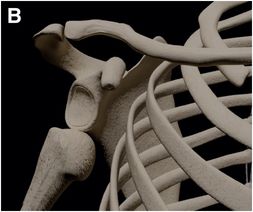

Anterior dislocations are most commonly the result of hyperflexion with the arm in abduction and external rotation, often in association with an anteriorly directed force onto the posterior aspect of the shoulder.
Injuries associated with anterior shoulder dislocation
Hill–Sachs lesion
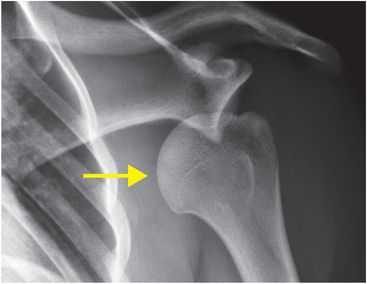
The Hill–Sachs lesion is an impaction fracture of the posterolateral humeral head, caused by contact of the humeral head upon the anterior-inferior glenoid after dislocation. Stryker notch radiograph of the shoulder (upper image) demonstrates a depression in the posterolateral humeral head (arrow), consistent with a Hill–Sachs lesion. AP radiograph in a different patient (lower image) demonstrates a Hill–Sachs lesion as linear sclerosis of the superolateral humeral head (arrow).

Anterior-inferior glenolabral complex injury
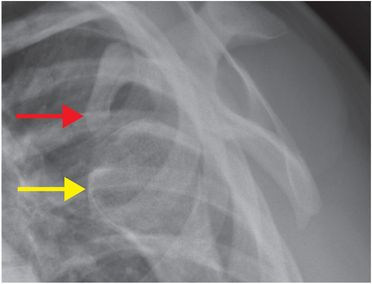
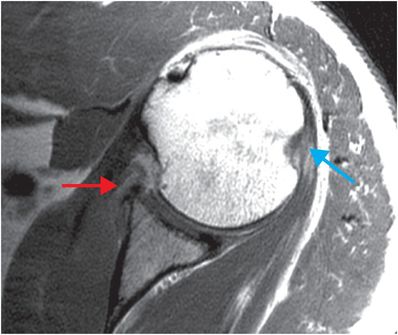
A Bankart lesion is an injury to the anterior-inferior glenoid labrum caused by impaction of the humeral head after dislocation. The glenoid is intact with a soft tissue Bankart injury, while a bony Bankart includes an avulsion fracture of the anterior-inferior glenoid rim. West Point radiograph of the shoulder (upper image) demonstrates a slightly displaced fracture of the anterior glenoid rim (yellow arrow), suggestive of a Bankart fracture due to prior anterior shoulder dislocation. Axial T1-weighted MR image of the shoulder in a different patient demonstrates an anterior-inferior labral tear consistent with a Bankart lesion (red arrow), and a partially imaged Hill–Sachs lesion (blue arrow).
Greater tuberosity fracture
Greater tuberosity fractures are often associated with anterior dislocation and are relatively uncommon in isolation. There may be limitation in functional ability if there is significant displacement of the fracture. Treatment is typically operative, with repair of the often-concomitant rotator cuff tear. AP radiograph demonstrates anteromedial shoulder dislocation with a displaced greater tuberosity fracture (arrow).
Imaging of glenohumeral dislocation
Initial pre-reduction radiographs should be obtained to verify diagnosis and to evaluate for the presence of any abnormality that may complicate reduction, such as a large loose bone fragment or comminuted glenoid fracture.
Stryker notch and West Point views can be obtained for optimal radiographic evaluation of Hill–Sachs and osseus Bankart injuries, respectively.
MRI can be obtained in suspected massive rotator cuff tear, or if there is concern for significant soft tissue interposition complicating reduction.
Suspected vascular injuries may require emergent CT angiography.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


