
Diagnosis: Segond fracture with complete tears of the anterior cruciate and medial collateral ligaments
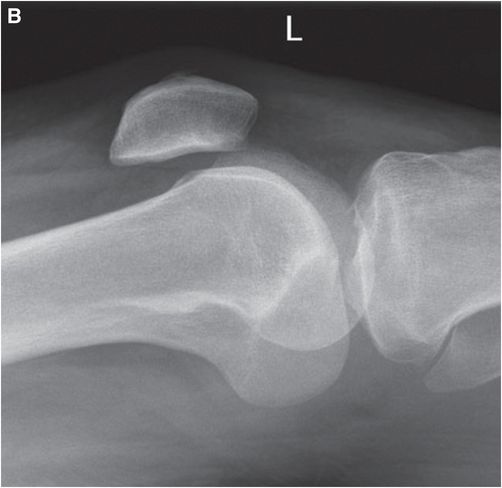
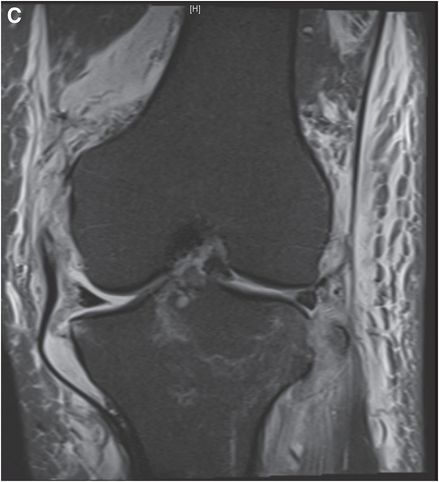
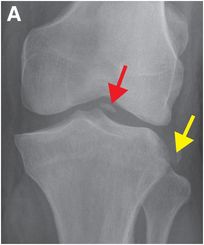
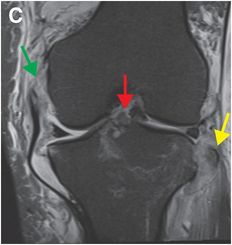
Frontal knee radiograph (A) demonstrates an avulsion fracture of the lateral tibial rim (Segond fracture; yellow arrow) and a fracture of the tibial eminence (red arrow). Cross-table lateral radiograph of the knee (B) shows a fat–fluid level, or lipohemarthrosis (blue arrow), indicating concomitant intra-articular fracture with leakage of marrow fat into the joint capsule. Coronal proton density fat-suppressed (C) and sagittal proton density (D) MR images show complete tears of the femoral attachment of the medial collateral ligament (green arrow) and anterior cruciate ligament (white arrow). The Segond fracture (yellow arrow) and avulsed tibial spine (red arrow) are also seen on the coronal image. There is focal bone narrow edema of the trochlea (black arrow).


Discussion
A fracture of the non-articular surface of the lateral tibial rim is called a Segond fracture.
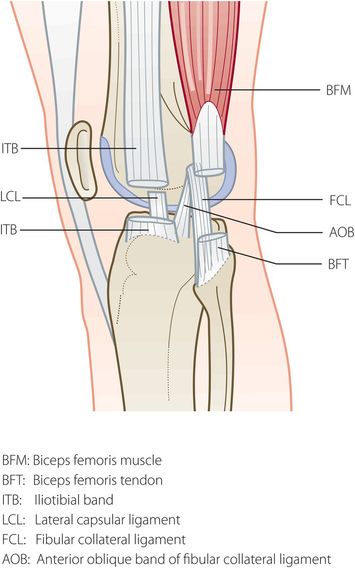
The site of a Segond fracture is posterior and just proximal to Gerdy’s tubercle, which is the tibial attachment of the iliotibial band.
Opinion varies about the exact anatomic components involved in this injury. Paul Segond, who identified the injury in 1879 before the advent of x-rays, believed it was the result of avulsion of the central portion of the lateral capsular ligament. Since then, injury to the posterior fibers of the iliotibial band and the anterior oblique band of the fibular collateral ligament has been postulated, although the exact structures involved remain controversial.
Segond fractures may be inconspicuous, but are essential to recognize, as the fracture is associated with extensive ligamentous injury and lateral knee instability. If the fracture is not initially identified and appropriately treated, chronic instability can occur.
Radiographs are the initial imaging modality for detecting a Segond fracture. Once it has been identified by plain film, subsequent MRI is essential to evaluate for associated injuries, including:
anterior cruciate ligament (ACL) tears (most common, in 75–100% of cases)
medial or lateral meniscal tears (in 66–75% of cases)
other avulsion injuries including avulsion of the fibular head, tibial spine, and Gerdy’s tubercle
posterolateral corner injuries
Clinical synopsis
The patient was discharged from the Emergency Department with a hinged knee brace and instructions for immobilization. He did well with conservative treatment.
Self-assessment
|
|
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


