Diagnosis: Schatzker type VI tibial plateau fracture, proximal fibular fracture, and traumatic popliteal arterial dissection
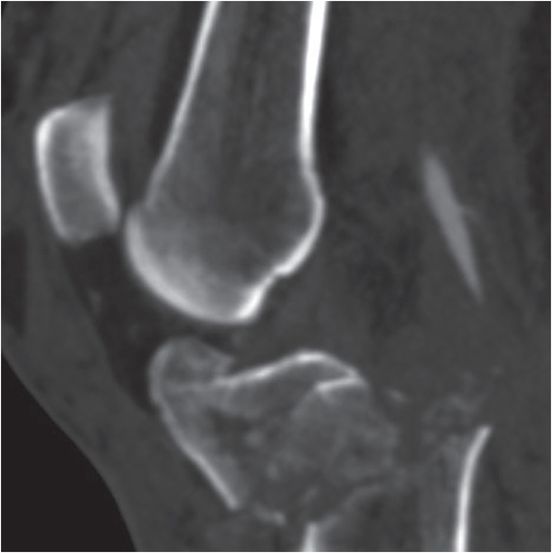
AP radiograph of the knee demonstrates a comminuted bicondylar fracture of the tibial plateau, transverse fracture of the tibial metaphysis, and a fracture of the proximal fibula. Sagittal CT angiogram demonstrates smooth short segment tapering with complete distal occlusion of the popliteal artery (arrow).


Discussion
Imaging of tibial plateau fractures
Radiographs are the initial imaging evaluation of knee trauma. Some tibial plateau fractures can be missed or difficult to identify by radiography. The presence of a lipohemarthrosis on the cross-table lateral view should prompt further evaluation by CT to detect a radiographically occult fracture. A subtle band of sclerosis of the medial or lateral tibial plateau may indicate an impacted fracture.
While plain radiographs are typically the initial imaging modality for assessing for fractures, these often underestimate fracture extent, depression, and grade. Cross-sectional imaging with MR or CT is the standard of care for assessing tibial plateau fractures seen on radiographs. MR can detect associated ligamentous and tendinous injuries. CT angiography is used to assess for vascular compromise or when there is clinical suspicion of compartment syndrome.
Grading of tibial plateau fractures
The most widely used grading system for fractures of the articular surface of the tibial plateau is the Schatzker classification. Schatzker categories range from I to VI, with higher grades indicating increased severity and worse prognosis. As the grade increases, the likelihood of damage to menisci, ligaments, neurovascular structures, and soft tissues increases.
Types I through III typically occur due to low-energy injury and management centers on repairing damaged articular cartilage and stabilizing the tibial plateau. Types IV through VI typically occur as a result of high-energy injury and management centers both on repairing soft tissue damage and bony stabilization.
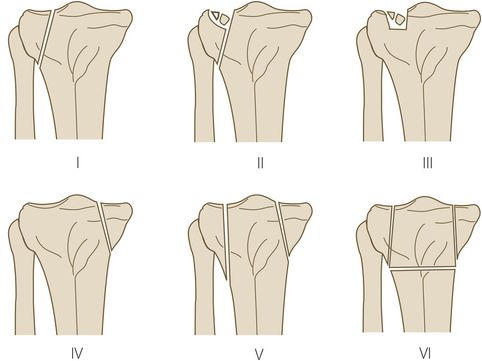
Type I: lateral split fracture with little (less than 4 mm) or no depression
Type II: lateral split fracture with depression
Type III: compression fracture of the articular surface
Type IV: medial split fracture with or without depression
Type V: bicondylar split fracture
Type VI: bicondylar split fracture with transverse fracture of metaphysis
Clinical synopsis
This patient, a 52-year-old male with a Schatzker grade VI fracture and popliteal artery dissection, was admitted and underwent fasciotomies, a popliteal bypass, external fixation, and multiple soft tissue debridements. A limb salvage and ORIF of the complex fracture was attempted; however, a transfemoral amputation was ultimately necessary.
Self-assessment
|
|
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


