Diagnosis: Medial (tibial) hallux sesamoid fracture and tear of the plantar plate and medial sesamoid-phalangeal ligament (turf toe)
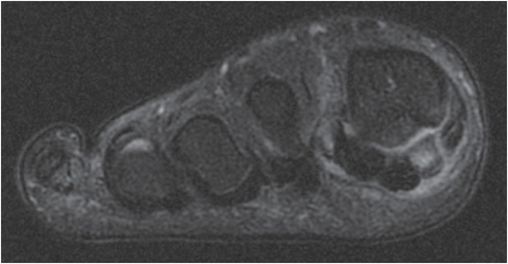
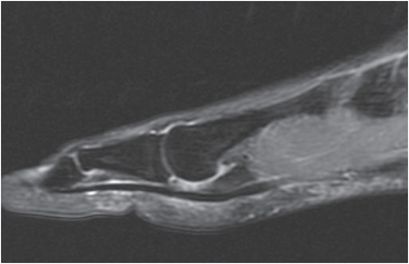
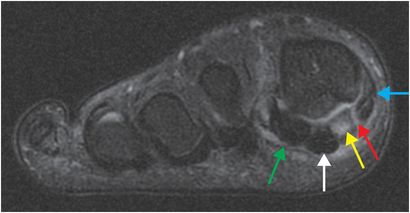
Frontal radiograph of the right foot (upper image) demonstrates two distracted components of the fractured medial sesamoid (yellow arrows). Sharp margination of the apposing cortices suggests acute transverse fracture. Coronal T2-weighted MR with fat suppression (lower left image) reveals focal marrow edema in the fractured medial sesamoid (yellow arrow) with surrounding edema. There is linear increased signal (red arrow) at the attachment of the abductor hallucis to the medial sesamoid, consistent with tear. There is a tear of the medial sesamoid–phalangeal ligament (blue arrow). The lateral sesamoid (green arrow) and flexor hallucis longus tendon (white arrow) are intact. Sagittal STIR MR image demonstrates a torn plantar plate (orange arrow).


Discussion
Sesamoids are seed-like bones (the word “sesamoid” is derived from a Greek word meaning “resembling a sesame seed”) that are embedded in tendons, typically spanning a joint.
The sesamoids absorb shock, prevent tendon damage, and enhance joint gliding. Hallucal sesamoids associated with the great toe are prone to injury due to the large forces transmitted through them during gait.
There are two hallucal sesamoids; the medial (tibial) sesamoid and the lateral (fibular) sesamoid. They are embedded in the flexor hallucis brevis tendon that spans the first metatarsophalangeal (MTP) joint in the plantar plate.
Fractures usually relate to sudden loading of the forefoot as might occur from jumping or falling from height. Abnormal ossification can lead to a partite configuration that can be difficult to differentiate from fracture.
Tenuous blood supply to sesamoids has been implicated in conditions such as avascular necrosis and delayed healing or nonunion of fractures.
Turf toe injuries are a spectrum of injuries of the plantar capsuloligamentous–sesamoid complex.
The abductor hallucis tendon inserts on the medial sesamoid with fibers contributing to the medial capsule.
The adductor hallucis muscle contributes fibers to the lateral sesamoid, capsule, and plantar plate.
Flexor hallucis brevis inserts on the sesamoids, while flexor hallucis longus runs in between the plantar aspect of the sesamoids to continue to the distal phalanx.
The medial and lateral sesamoid–phalangeal ligaments are stabilizing structures.
Imaging of sesamoid injury
Standard weightbearing radiographs are typically the initial imaging modality to assess bone morphology and exclude other causes of first metatarsal pain.
If an abnormality is suspected or if there is a high suspicion for sesamoid injury, then dedicated sesamoid axial and/or oblique stress radiographs can provide optimal visualization.
Bone scan is a sensitive but nonspecific imaging modality. Both feet should be imaged to evaluate for abnormal asymmetric uptake. It is important to note that bone scan may show physiologically increased, symmetric uptake in asymptomatic patients.
CT is useful to assess osseous detail in fractures and avascular necrosis, while the role of MRI is to detect marrow signal abnormality and evaluate the integrity of associated ligaments and tendons.
Clinical synopsis
Radiographs of the contralateral foot were obtained to exclude traumatic distraction of a bipartite medial sesamoid. The patient underwent open reduction and internal fixation of the medial sesamoid with reconstruction of the first MTP joint. In isolated sesamoid fracture, conservative therapy, such as non-weightbearing for several weeks, is commonly prescribed. Noncompliance can lead to complications such as avascular necrosis.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
72 67-year-old female with shoulder pain and limited range of motion following a fall onto an outstretched hand
 35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
35 37-year-old woman with a history of rheumatoid arthritis presenting with non-resolving bilateral effusions and chest pain
 62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
62 38-year-old male complaining of diffuse abdominal pain after a motor vehicle collision
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


