CASE 9 A 2-year-old child presents with partial-onset seizures, microcephaly, severe developmental delay, and quadriparesis. Figure 9A Figure 9B Figure 9C Figure 9D Axial T1- (Fig. 9A), axial T2- (Fig. 9B), and coronal T2-weighted (Fig. 9C) images show bilateral, asymmetrical, large open clefts in both hemispheres. The surface opening is well depicted on the surface rendering of the left hemisphere (Fig. 9D). The septum pellucidum is absent. The clefts are lined with a somewhat thick, irregular, polymicrogyric cortex that extends to the lateral ventricles. The cortex surrounding the clefts also looks polymicrogyric. Surface rendering shows the cortical sulci converging toward the defect. The corpus callosum is thin posteriorly, presumably by lack ofcorresponding cortex with which to connect. Over the fluid-filled cavity of the large cleft on the right, the vault is thinned and expanded. Bilateral schizencephaly, open-lipped type Schizencephaly is defined as a congenital brain cleft, which extends from the pial to ventricular surface (transmantle defect) and is lined by dysplastic cortex joining the lateral ventricles. The etiology is usually unknown. The clinical finding of schizencephaly is cerebral palsy in which the psychomotor defect is related to the location of the lesion. Epilepsy develops in ~50% of cases. The severity of clinical presentation is dependent on the extent of the abnormality.
Clinical Presentation
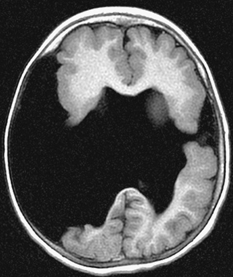

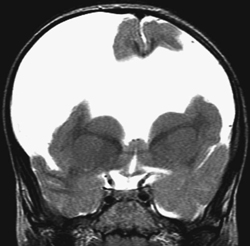
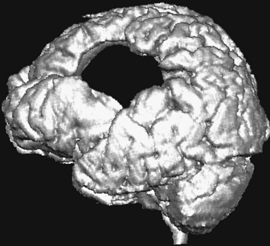
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Clinical Findings
Pathology
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


