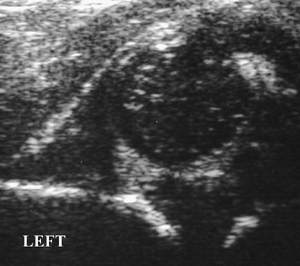
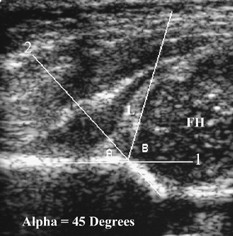
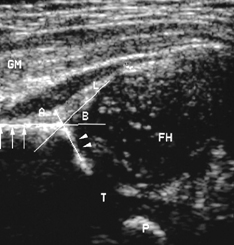
CASE 92 A 1-week-old female is referred with a positive Ortolani test. Figure 92A Figure 92B Standard coronal ultrasonographic exam of both hips shows a shallow acetabulum on the left (Fig. 92B) compared with the normal right (Fig. 92A). The left femoral head epiphyseal center is dislocated superolaterally with an elevated echogenic labrum. Figure 92C Coronal sonogram of the hip depicts superolateral subluxation of the femoral head (FH). There is uplifting of labrum (L). The a angle (A) is formed by a line drawn parallel to the straight iliac echo (line 1) and a crossing line (line 2) drawn parallel to acetabular echogenic margin. Figure 92D Coronal hip sonogram depicts femoral head (FH) well covered by echogenic labrum (L). Alpha (A) and β (B) angles are within normal limits. The deepest portion of the acetabulum is demonstrated based on visualization of triradiate cartilage. Gluteus medius (GM) spans hip joint in coronal plane. Arrows depict echogenic iliac margin. Arrowheads depict cartilaginous acetabulum. Developmental dysplasia of the hip (DDH) with dislocation Dislocation related to: DDH constitutes a spectrum of abnormalities ranging from minor neonatal instability to frank irreducible dislocation. The disorder is dynamic, with the potential to improve or worsen over time, and evolves prenatally (36–40 weeks) or postnatally (98%). The remaining cases are teratogenic, initiating early in development of the fetal hip. The incidence of hip instability detected at birth is 1 to 2%; however, the vast majority of these cases reflect transient instability and resolve. The quoted incidence of DDH is ~1 in 1000. Girls have a significantly higher incidence compared with boys (5:1). Lack of fetal mobility as seen in breech presentations has associated DDH in up to 23%. Two thirds of cases involve first-born children, with an overall familial incidence of 20%. The cause of DDH appears multifactorial with a combination of genetic, hormonal, and positional factors playing a role. A lack of congruent mutual development of the femoral head and acetabulum can lead to insufficient coverage of the femoral head by the acetabulum with resulting altered mechanicswith the application of stress/movement. This may be the result of ligamentous laxity or underlying acetabular dysplastic changes. The natural history of DDH is variable. More than 90% of these hips stabilize over the first 2 to 3 weeks after birth, whereas a minority will go on to either sublux or dislocate. Others will remain located in an abnormally shaped acetabulum termed acetabular dysplasia.
Clinical Presentation

Imaging Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Clinical Findings
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


