Case presentation
A 7-week-old male presents with difficulty breathing while feeding for 1 day. The child is formula fed 3 ounces every 3–4 hours, but over the past 2–3 days, he has been feeding every 4 hours and not completing the 3 ounces. One day ago, he developed increased work of breathing while feeding and “turned pale for several seconds” according to the parents. There was no associated tonic-clonic activity with this event and the child did not stop breathing. This continued with most of the feeds during the day but otherwise there were no other concerns. On the day of presentation, he “turned blue for a few seconds” while feeding. With these episodes, the mother reports nasal congestion and copious oral secretions (with some formula) that she has been suctioning with a bulb syringe. There has been no fever, vomiting, diarrhea, rash, or known trauma, and the child is reported otherwise to be at his baseline.
The child recently arrived from Central America. The parents report the child has not had problems with breathing or feeding in the past and has “been healthy.” There was little prenatal care but the mother was told the child “had a heart problem” on a prenatal ultrasound, but she did not understand what the issue was and was told “nothing could be done.” Aside from this, the parents report no other concerns or problems. They have not yet been to a local pediatrician.
The physical examination reveals an overall well-appearing, vigorous child who is in no acute distress. He is afebrile with a heart rate of 170 beats per minute, respiratory rate of 45 breaths per minute, and a pulse oximetry reading of 100% on room air. He has a completely normal examination; his cardiac examination demonstrates no heart murmur, rub, or click; he has equal pulses throughout and is well perfused.
Imaging considerations
Plain radiography and fluoroscopy
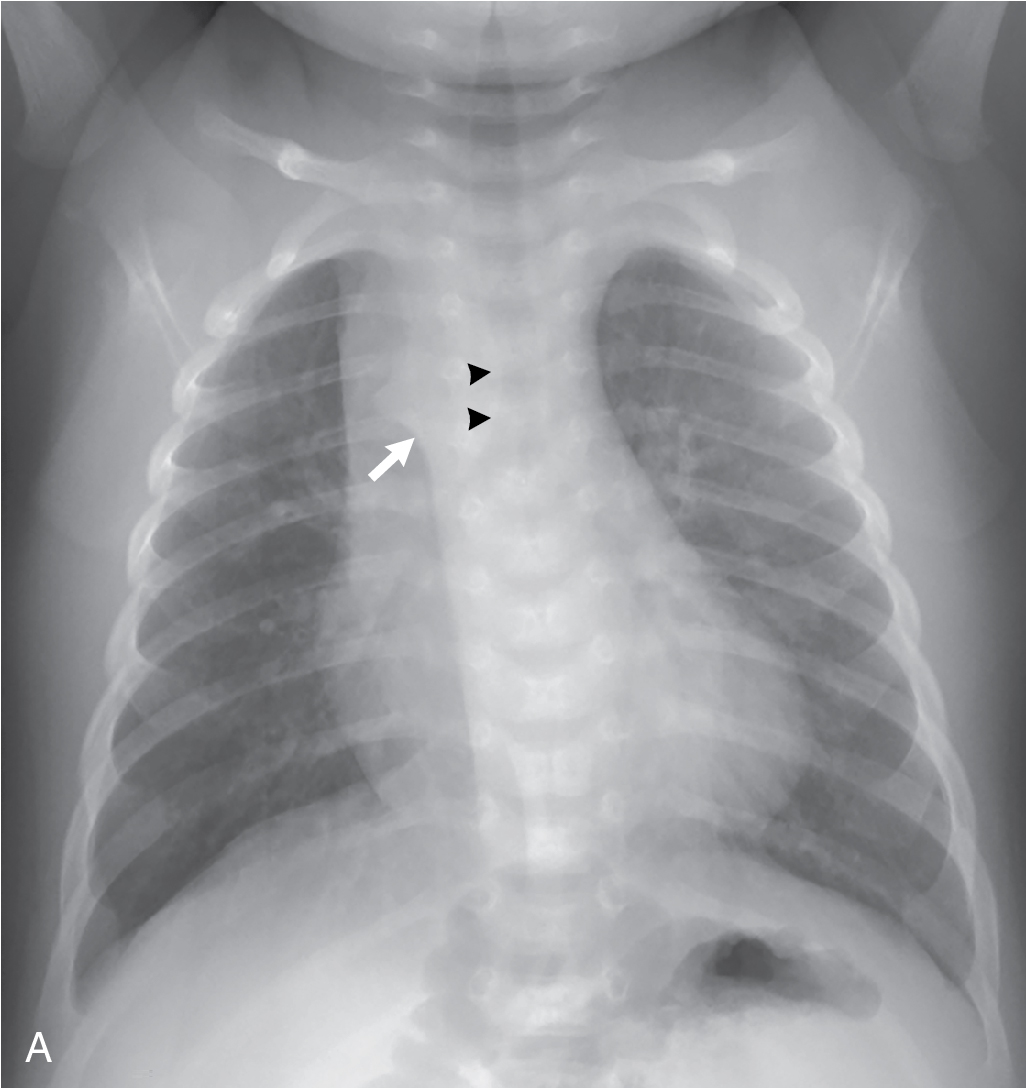
Chest radiography is often employed as a first-line resource in patients when there is concern for a cardiopulmonary process. In interpreting the chest radiograph, attention should be given to the side of the cardiac apex, the aortic arch, and the stomach bubble. In young infants and children, the aortic arch may not be directly visible, but its position is inferred by the appearance of the trachea. There is a mild mass effect upon the trachea from the side of the aortic arch, and the trachea mildly deviates or buckles away from the side of the aortic arch on a frontal view of the chest. If the position of the aortic arch is difficult to determine on chest radiograph, chest fluoroscopy can be utilized to determine aortic arch positioning. A fluoroscopic esophagram using barium contrast is useful in the evaluation for vascular rings and slings, in which developmental anomalies of the aortic arch and pulmonary artery can produce a mass effect upon the esophagus and trachea. A contrast esophagram performed for the evaluation of vascular anatomy should be performed by a practitioner experienced in pediatric imaging.
Echocardiography (echo)
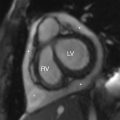
For suspected cardiac disease and aortic arch anomalies, echo is employed. Anatomy and function can be demonstrated. If very complex anatomy is discovered, and especially if aortic anatomy is not well delineated on echo, this may prompt the use of additional advanced imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI). Echo is resource dependent; expertise in the performance and interpretation of pediatric echo is needed to obtain a meaningful study and interpretation. Additionally, availability may restrict immediate or routine use in an emergent setting.
Computed tomography
This imaging modality is used as a secondary study when either plain radiography or echo is abnormal or inconclusive. CT angiography has been found to be useful to further delineate aortic arch anatomy. , The decision for CT utilization may be made after subspecialty consultation or in hospitalized patients undergoing further evaluation. Contrast-enhanced CT angiography of the chest is especially useful in the evaluation for aortic abnormalities, including aortic arch anomalies and aortic coarctation, as well as to evaluate pulmonary artery anatomy and systemic to pulmonary collateral vessels. Pediatric imaging expertise is necessary for the performance and interpretation of CT angiography for pediatric cardiovascular disease.
Magnetic resonance imaging
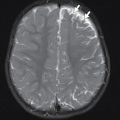
This modality is also typically obtained after initial imaging, such as chest radiography or an echocardiogram. MRI has the advantage of providing excellent anatomic detail and can be used to evaluate anomalies of the aortic arch, aortic coarctation, pulmonary artery anatomy, and cardiac anatomy and function. As with CT, subspecialty consultation should be considered before utilizing this imaging test. While MRI has the advantage of a lack of ionizing radiation, the length of time to complete the study often requires sedation in infants and young children. Pediatric imaging expertise is necessary for the performance and interpretation of pediatric cardiovascular MRI and magnetic resonance angiography.
Imaging findings
The history of an unknown heart problem, coupled with the development of decreased feeding and color change, prompted concerns for a worsening cardiac condition, although the physical examination was not concerning. A two-view chest x-ray series was obtained. This demonstrated a right-sided aortic arch with a cardiothymic silhouette that is in the upper range of normal in size ( Fig. 12.1 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


