Case presentation
An 11-year-old male presents with acute onset of left-sided lower abdominal pain and left-sided flank pain, which began 1–2 hours prior to presentation. The patient was not engaged in any particular activity; he states that he was “just relaxing” when the pain began. He denies trauma. There has been no fever, back pain, dysuria, hematuria, testicular pain/swelling, or other abdominal pain. While he has not had vomiting, he does report nausea.
The patient appears uncomfortable on physical examination but is not toxic. His vital signs show a temperature of 98 degrees Fahrenheit, a heart rate of 100 beats per minute, a respiratory rate of 22 breaths per minute, a blood pressure of 108/58 mm Hg, and a room air oxygen reading of 100%. His physical examination is unremarkable. He has no abdominal tenderness, rebound, or guarding; there is no costovertebral angle tenderness. The thoracic and lumbar spine exams are normal. His genital examination reveals Tanner stage II; there is no scrotal edema, erythema, or tenderness. He is circumcised. The inguinal area has no obvious masses and there is no tenderness.
Imaging considerations
Imaging is useful to determine not only the presence of nephrolithiasis but also associated complications, such as ureteral obstruction and hydronephrosis. The primary imaging modalities utilized during the evaluation of a pediatric patient with suspected nephrolithiasis are generally available, including ultrasound and computed tomography (CT).
Plain radiography
Plain radiography can detect radiopaque stones but has low sensitivity and specificity (62% and 67%, respectively). One study found plain radiography (a kidney-ureter-bladder image, or KUB) to be of limited value as a sole imaging modality for small renal stones, stones detected by KUB were mostly detected by ultrasound (US), and adding KUB to US did not improve the detection rate. Guidelines exist suggesting the use of a combination of US and plain radiography for following diagnosed renal stones, , but this remains somewhat controversial and is best left to the discretion of a consulting pediatric urologist. As a rule, plain radiography has little use in the acute detection and management of renal stones and is not typically utilized.
Ultrasound
US is the imaging modality of choice in pediatric patients with suspected nephrolithiasis, and the technology has improved over the past 10 years. , The lack of ionizing radiation and the general availability of this technique are attractive attributes. US is not as sensitive or specific for nephrolithiasis when compared to CT, with previous studies demonstrating a sensitivity of approximately 30%–50% compared to noncontrast CT. , Recent studies have found US to have a sensitivity and specificity of 70% and 100%, respectively, with the ability to detect clinically significant stones. , , Another study demonstrated a sensitivity of 67% with a high specificity (97%) compared with noncontrast CT, which is consistent with previously recently published literature. Notably, US has been shown to have a high detection rate (90%) for renal stones but a low rate (38%) for ureteral stones. ,
Computed tomography
CT is considered the gold standard for the detection of nephrolithiasis, with near 100% sensitivity and specificity. , , While this study is generally rapid and intravenous (IV) contrast is not needed, exposure of the pediatric patient to ionizing radiation is a concern. One study of nearly 8000 children found that, on average, pediatric patients received two CT scans for a single nephrolithiasis episode. In another study, CT use was noted to have increased and linked to various patient demographic factors (age, race, and insurance status), as well as strongly linked to the treating hospital, which was the single strongest factor. Due to improvement in US technology and techniques, CT can be used as a second-line study in patients with a high clinical and historical suspicion for nephrolithiasis but in whom US is nondiagnostic. , , ,
In an effort to reduce ionizing radiation exposure, professional societies have developed imaging recommendations: the American Urological Association (2012) and the European Association of Urology (2013) have both recommended ultrasonography as the first-line imaging modality in pediatric patients, with CT reserved for patients with equivocal US findings or negative US findings in the setting of a strong clinical suspicion for a renal stone. , , , , These recommendations are in keeping with the Society for Pediatric Radiology, the American College of Radiology, and the American Society of Radiologic Technologists Image Gently campaign to reduce ionizing exposure for pediatric patients.
Imaging findings
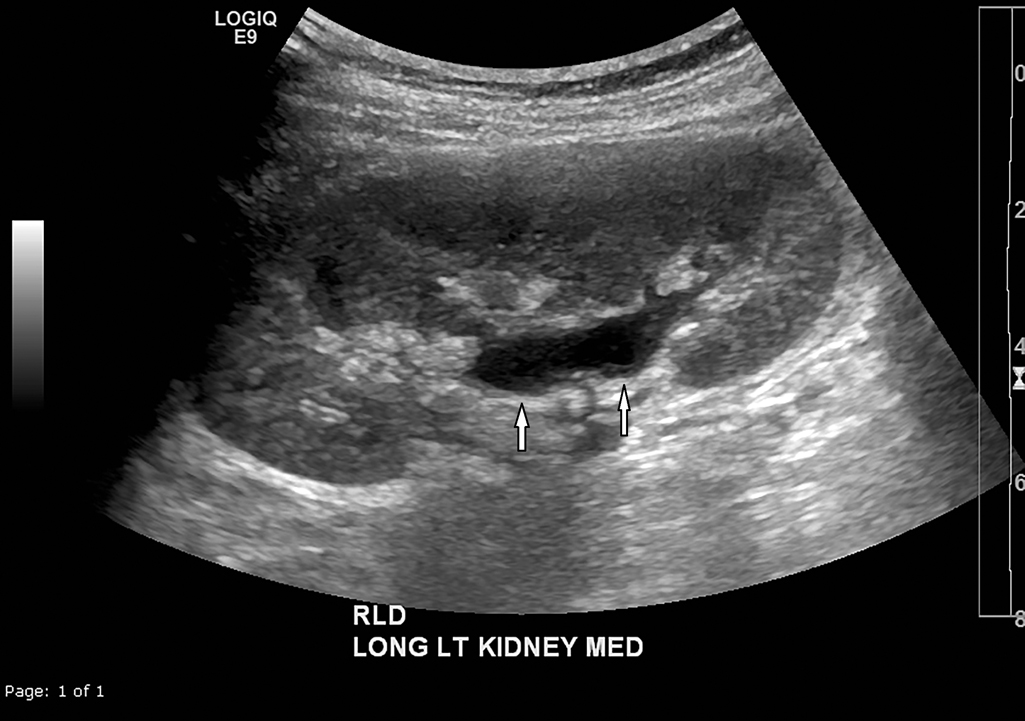
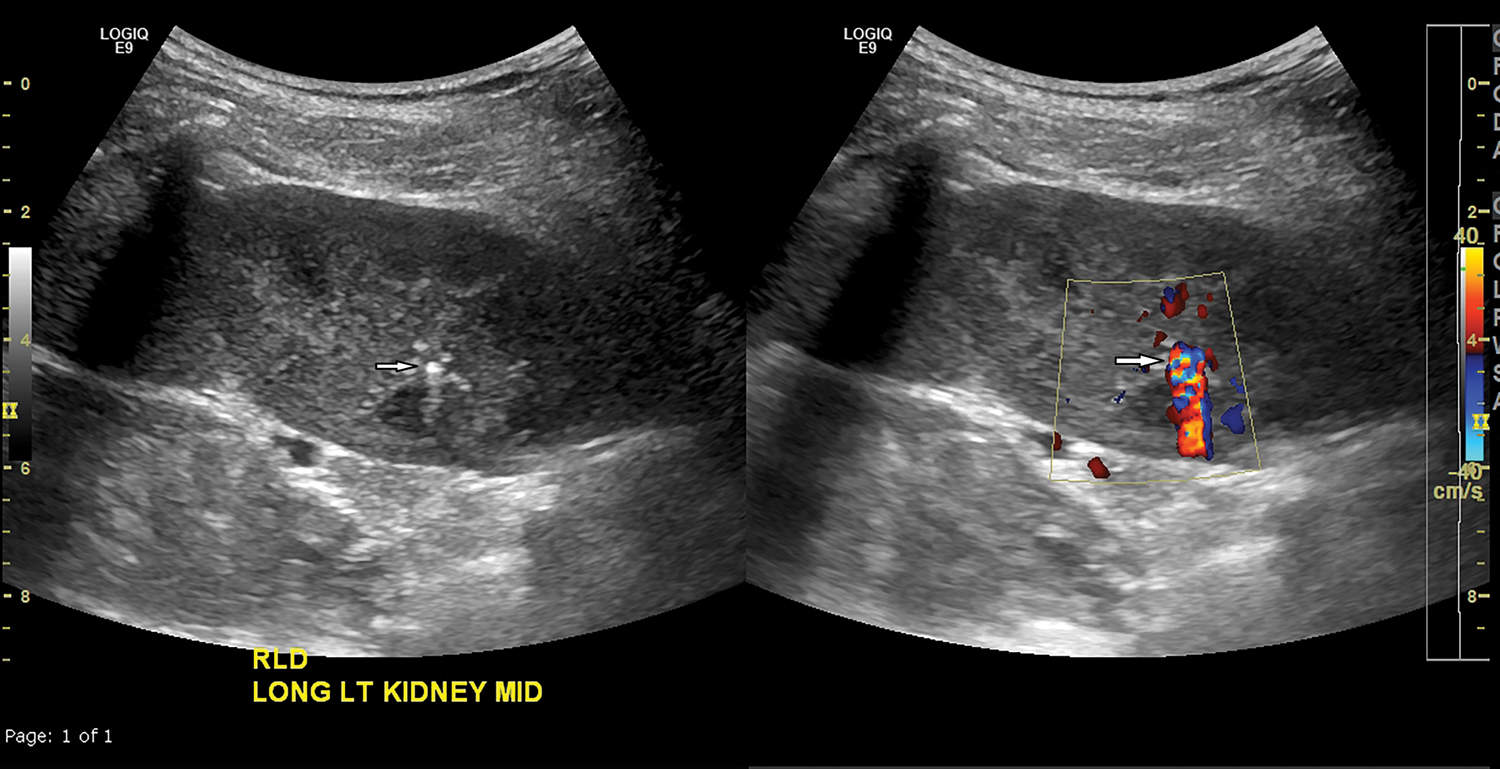
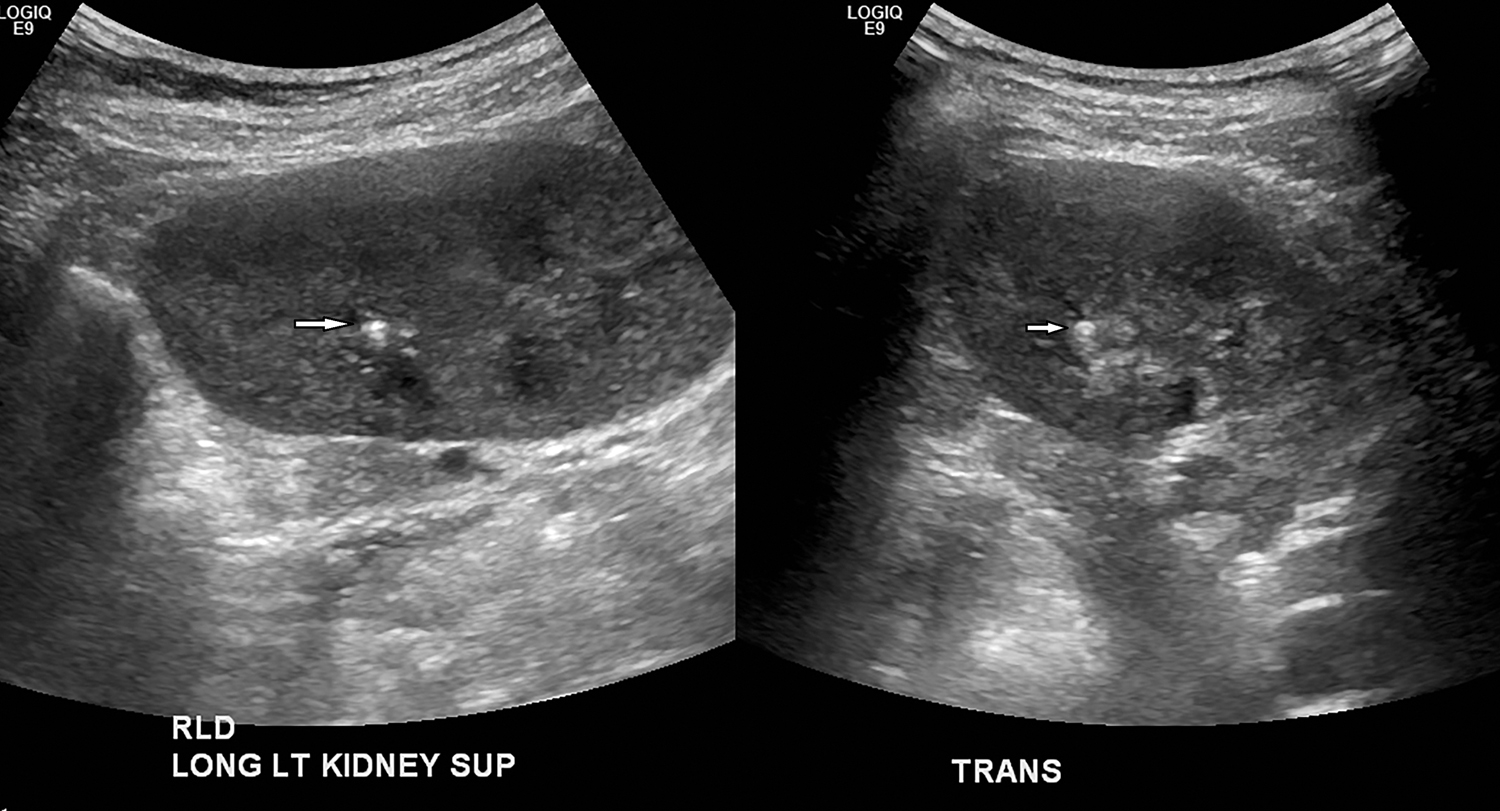
This patient underwent renal US. The right kidney is normal in size and echotexture, with normal corticomedullary differentiation, normal renal cortical thickness; the left kidney is normal in size and echotexture, with normal corticomedullary differentiation, normal renal cortical thickness ( Figs. 24.1–24.3 ). There is a 3-mm stone located in the upper pole of the left kidney and a 4-mm stone in the midportion of the kidney.
For comparison, another case is presented here. This child presented with right flank pain radiating to the right upper quadrant along with nonbilious, nonbloody emesis and nausea. An initial US did not demonstrate a renal stone, and due to clinical suspicion, a noncontrast CT scan was obtained. CT revealed a 2-mm stone in the distal right ureter, adjacent to the right ureterovesicle junction. The right ureter is mildly dilated with mild right hydronephrosis ( Figs. 24.4–24.6 ).










