



Abdomen Axial 1

Diagnostic Consideration
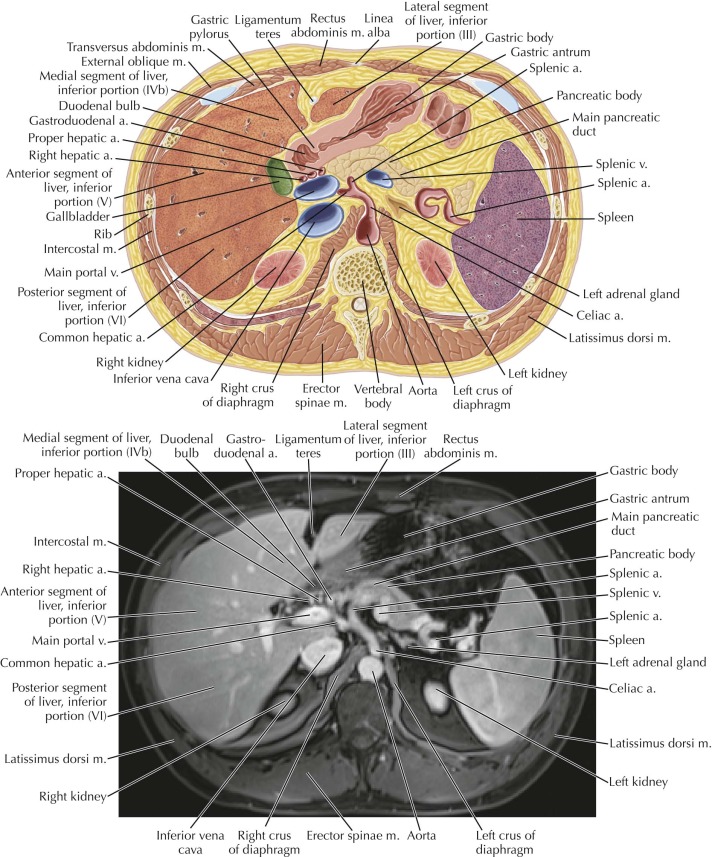
In magnetic resonance imaging (MRI), all signal intensity is relative; signal intensity varies depending on the type of MR sequence. High signal intensity on T1-weighted images is typically associated with fat, proteinaceous content, subacute hemorrhage, paramagnetic substances (e.g., melanin, gadolinium), and slow blood flow within vessels. High signal intensity on T2-weighted images is typically associated with fluid, including cerebrospinal fluid (CSF), urine, bile, gastric fluid, and enteric fluid, as well as fluid-filled lesions (cyst, cystic or necrotic tumor), hemangiomas, and fat. Low signal intensity on T1- and T2-weighted images is associated with susceptibility artifact from gas, iron, and metallic objects, as well as fibrous tissue, cortical bone, and fast blood flow within vessels.

Abdomen Axial 2

Normal Anatomy
Many systems have been proposed for liver segmentation anatomy. The approach most frequently used, however, is the Couinaud system, which subdivides the liver into eight functionally independent segments (I-VIII). Portal triads, composed of branches of the portal vein, hepatic artery, and biliary ducts, are seen within the center of each segment, whereas hepatic veins are seen in the periphery. Because each hepatic segment is self-contained, a single segment can be surgically resected without injury to the remaining segments.
In this system, a transverse plane through the level of the main portal vein divides the liver into lateral, medial, anterior, and posterior segments, each with superior and inferior portions, as follows:
The right hepatic vein divides the right hepatic lobe into an anterior segment with superior (VIII) and inferior (V) portions and a posterior segment with superior (VII) and inferior (VI) portions.
The middle hepatic vein (superiorly) and gallbladder fossa (inferiorly) divide the liver into right and left hepatic lobes.
The left hepatic vein (superiorly) and left intersegmental fissure (inferiorly) divide the left hepatic lobe into a medial segment with superior (IVa) and inferior (IVb) portions and a lateral segment with superior (II) and inferior (III) portions.
Segment I, the caudate lobe of the liver, is located posteriorly, adjacent to the intrahepatic portion of the inferior vena cava (IVC).

Abdomen Axial 3

Normal Anatomy
The ligamentum venosum, a remnant of the obliterated ductus venosus, travels within a fissure along the inferior surface of the liver between the caudate lobe and left hepatic lobe. In utero, the ductus venosus shunts oxygenated blood from the umbilical vein directly into the fetal IVC. After birth, neonatal circulation takes over, and the umbilical vein and ductus venosus close.



Abdomen Axial 5

Normal Anatomy
The ligamentum venosum is in continuity with the ligamentum teres, a remnant of the obliterated umbilical vein. The ligamentum teres travels in the fissure for the ligamentum teres, located in the lower third of the left intersegmental fissure, then courses within the falciform ligament toward the umbilicus (see also Axial 6 ).

Abdomen Axial 6

Pathologic Process
An enlarged paraumbilical vein may become visible in the patient with portal hypertension, allowing for portosystemic venous collateralization within the anterior abdominal wall and producing the characteristic appearance of caput medusae. This venous collateral is distinct from the obliterated umbilical vein.

Abdomen Axial 7
Normal Anatomy
On T1-weighted MR images, the normal pancreas has the highest signal intensity relative to other parenchymal organs, because of its high protein and rough endoplasmic reticulum content, followed by the liver, then the spleen. On T2-weighted images, the pattern is reversed; the normal spleen has higher signal intensity than the liver or pancreas. Fat is hyperintense on both T1- and T2-weighted images relative to skeletal muscle, whereas fluid is hyperintense on T2-weighted images relative to skeletal muscle.



Abdomen Axial 9

Pathologic Process
Compression of the left renal vein as it passes between the aorta and superior mesenteric artery (SMA) can result in an outflow obstruction and left renal vein hypertension, referred to as nutcracker syndrome (or nutcracker phenomenon). In addition to compression of the left renal vein, look for perirenal varices and a unilateral left varicocele. Patients can present with left flank pain and hematuria, clinically mimicking symptoms of a left ureteral calculus. Note that nutcracker syndrome is distinct from the superior mesenteric artery syndrome, in which compression of the 3rd portion of the duodenum by the aorta and SMA can occur.



Abdomen Axial 11

Normal Anatomy
In the kidneys, the renal cortex demonstrates higher signal intensity compared with the renal medulla on T1-weighted MR images. On T2-weighted images, however, the renal medulla demonstrates higher signal intensity than the renal cortex because of higher fluid content.

Abdomen Axial 12

Normal Anatomy
The erector spinae muscles are composed of the iliocostalis muscles (laterally), the longissimus muscles (intermediate in location), and the spinalis muscles (medially, adjacent to spinous processes of vertebrae). On MR imaging, the fascial planes separating these muscles are difficult to discern and thus these muscles are collectively referred to as the “erector spinae muscles.”



Abdomen Coronal 2











