Abnormalities of the Superficial Peroneal Nerve at the Ankle
Anatomic Considerations
The common peroneal nerve is one of the two major continuations of the sciatic nerve, the other being the tibial nerve. The common peroneal nerve, which is also known as the common fibular nerve, provides sensory innervation to the inferior portion of the knee joint, and the posterior and lateral skin of the upper calf. The common peroneal nerve is derived from the posterior branches of the L4, L5, and S1 and S2 nerve roots. The nerve splits from the sciatic nerve at the superior margin of the popliteal fossa and descends laterally behind the head of the fibula (Fig. 12.1). The common peroneal nerve is subject to compression at this point by circumstances such as improperly applied casts and tourniquets. The nerve is also subject to compression as it continues its lateral course, winding around the fibula through the fibular tunnel, which is made up of the posterior border of the tendinous insertion of the peroneus longus muscle and the fibula itself. Just distal to the fibular tunnel, the nerve divides into its two terminal branches, the superficial and the deep peroneal nerves (Fig. 12.2). These branches are also known as the superficial and the deep fibular nerves. Each of these branches is subject to trauma and may be blocked individually with local anesthetic as a diagnostic and therapeutic maneuver.
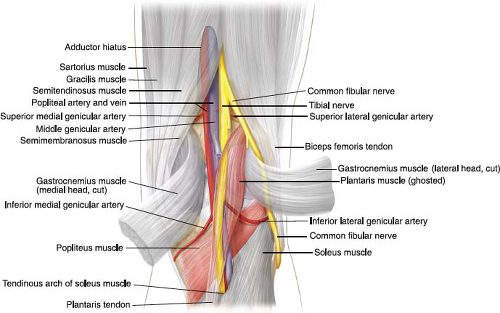 FIGURE 12.1 The common peroneal nerve is one of the two major continuations of the sciatic nerve, the other being the tibial nerve. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:117.) |
The deep branch continues down the leg in conjunction with the tibial artery and vein to provide sensory innervation to the web space of the first and second toes and adjacent dorsum of the foot (Fig. 12.3). Although this distribution of sensory fibers is small, this area is often the site of Morton’s neuroma surgery and thus is important to the regional anesthesiologist. The superficial peroneal nerve provides motor innervation to
all of the toe extensors and the anterior tibialis muscles. The superficial peroneal nerve passes beneath the dense superficial fascia of the ankle, where it is subject to an entrapment syndrome known as the anterior tarsal tunnel syndrome. The superficial peroneal nerve also provides sensory innervation to the toes except for the area between the first and second toe, which is supplied by the deep peroneal nerve (Fig. 12.4).
all of the toe extensors and the anterior tibialis muscles. The superficial peroneal nerve passes beneath the dense superficial fascia of the ankle, where it is subject to an entrapment syndrome known as the anterior tarsal tunnel syndrome. The superficial peroneal nerve also provides sensory innervation to the toes except for the area between the first and second toe, which is supplied by the deep peroneal nerve (Fig. 12.4).
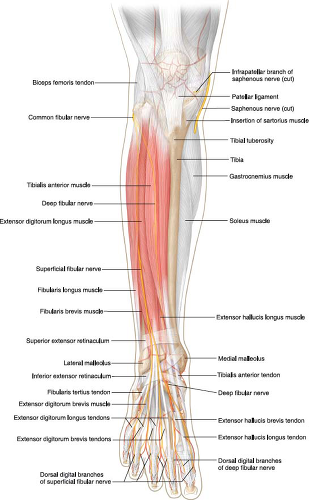 FIGURE 12.2 Just distal to the fibular tunnel, the common peroneal nerve divides into its two terminal branches, the superficial and the deep peroneal nerves. These branches are also known as the superficial and the deep fibular nerves. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:125.) |
 FIGURE 12.3 The anatomy of the distal superficial peroneal nerve. Note the relationship of the nerve to the superficial peroneal vein. |
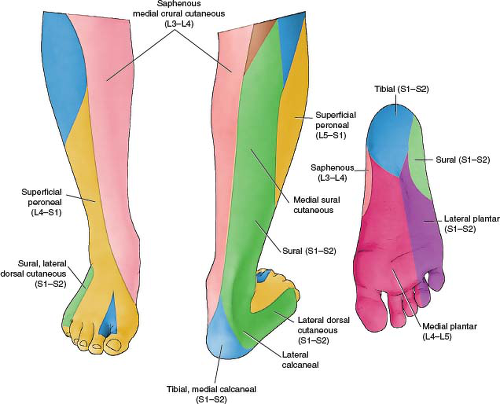 FIGURE 12.4 Sensory distribution of the distal superficial peroneal nerve. |
Clinical Correlates
The superficial peroneal nerve and its branches are the most commonly injured nerves of the ankle and foot with the average age of patients suffering from this problem being 28 years. Occurring equally in males and females, superficial peroneal neuropathy and entrapment is most commonly seen in runners, hockey, tennis, and racquetball players. Tight ice skates and ski boots have also been implicated in the evolution of this common sports injury. Other common causes of superficial peroneal neuropathy include compression and/or injury by ganglion cysts, tumors, fibular fractures, tenosynovitis, aberrant muscles, penetrating injuries, compartment syndromes, ankle edema, and ankle sprains (Figs. 12.5 and 12.6). The nerve is occasionally injured during ankle arthroscopy.
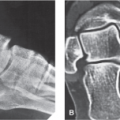
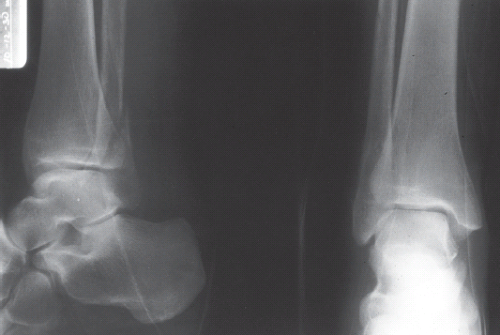 FIGURE 12.5 Radiographs demonstrating a fracture of the distal fibula. (From Bucholz RW, Heckman JD. Rockwood & Green’s Fractures in Adults. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.) |
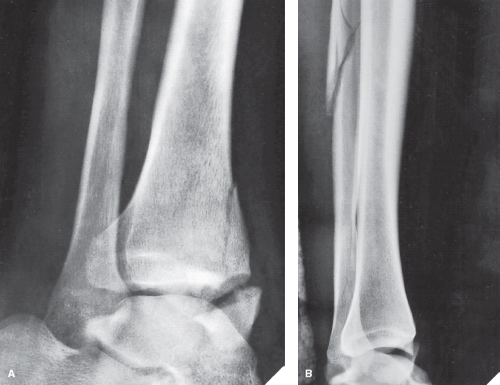 FIGURE 12.6 Maisonneuve fracture. A 22-year-old man injured his right ankle in a skiing accident. A: Oblique radiograph of the ankle shows a comminuted fracture of the medial malleolus, with extension into the anterior lip of the tibia. B: On the lateral view, a comminuted fracture of the fibula is apparent. This is a characteristic of a Maisonneuve-type fracture. (From Greenspan A. Lower limb III: ankle and foot. In: Orthopedic Imaging: A Practical Approach. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:340.) |
 FIGURE 12.7 The most common site of entrapment of the superficial peroneal nerve is the point at which it exits from the deep fascia. Impingement by the edge of the fascia alone or in combination with muscle herniation from beneath the edge of the fascia is responsible for compromise of the nerve. There will often be point tenderness as this point lies 9 to 12 cm above the most distal portion of the fibula.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|