Arthritis and Other Abnormalities of the Ankle Joint
Anatomic Considerations
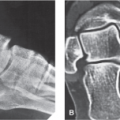
The ankle joint, which is also known as the tibiotalar or tibiocrual joint, is a synovial hinge-type joint that allows dorsiflexion and plantar flexion. The joint is composed of three bones: the tibia, the fibula, and the talus (Fig. 1.1). The tibia and fibula articulate with the talus at the ankle joint. The articular surface is dome shaped and is referred to as the mortise (Fig. 1.2). The articular surfaces are covered with hyaline cartilage, which are susceptible to arthritis. The joint is completely surrounded by a dense capsule that provides support to the joint. The majority of strength to the ankle joint is provided by the major ligaments which include the deltoid, anterior talofibular, calcaneofibular, and posterior talofibular ligaments (Fig. 1.3). The joint capsule is lined with a synovial membrane that attaches to the articular cartilage and may give rise to bursae. The tibiotalar joint is innervated by the deep peroneal and tibial nerves. In addition to arthritis, the joint is susceptible to the development of tendinitis, bursitis, fractures, and disruption of the ligaments, cartilage, and tendons.
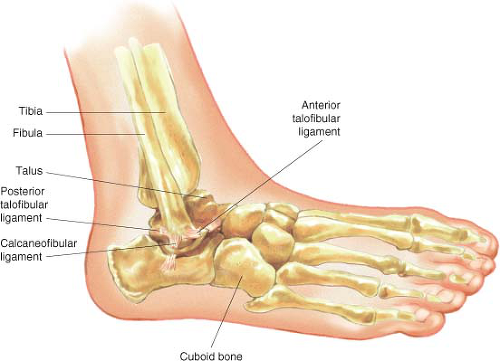 FIGURE 1.1 The articulations of the ankle joint. |
Clinical Correlates
The ankle joint’s articular cartilage is susceptible to damage, which will result in arthritis with its associated pain and functional disability if left untreated (Fig. 1.4). Osteoarthritis of the
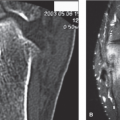
joint is the most common form of arthritis that results in ankle joint pain and functional disability, with rheumatoid arthritis and posttraumatic arthritis also causing arthritis of the ankle joint. The ankle joint is the most commonly injured joint in the human body, with sports injuries from basketball, football, tennis, and cross country running being frequent causes of pain and functional disability. Less common causes of arthritis-induced ankle joint pain include the collagen vascular diseases, infection, villonodular synovitis, and Lyme disease (Fig. 1.5). Acute infectious arthritis of the ankle joint is best treated with early diagnosis, with culture and sensitivity of the synovial fluid, and prompt initiation of antibiotic therapy. The collagen vascular diseases generally manifest as a polyarthropathy rather than a monoarthropathy limited to the ankle joint, although ankle pain secondary to the collagen vascular diseases responds exceedingly well to ultrasound-guided intra-articular injection of the ankle joint.
joint is the most common form of arthritis that results in ankle joint pain and functional disability, with rheumatoid arthritis and posttraumatic arthritis also causing arthritis of the ankle joint. The ankle joint is the most commonly injured joint in the human body, with sports injuries from basketball, football, tennis, and cross country running being frequent causes of pain and functional disability. Less common causes of arthritis-induced ankle joint pain include the collagen vascular diseases, infection, villonodular synovitis, and Lyme disease (Fig. 1.5). Acute infectious arthritis of the ankle joint is best treated with early diagnosis, with culture and sensitivity of the synovial fluid, and prompt initiation of antibiotic therapy. The collagen vascular diseases generally manifest as a polyarthropathy rather than a monoarthropathy limited to the ankle joint, although ankle pain secondary to the collagen vascular diseases responds exceedingly well to ultrasound-guided intra-articular injection of the ankle joint.
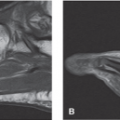
 FIGURE 1.2 A, B: The articular surface of the tibiotalar joint is dome shaped. (From Berquist TH. Fractures/dislocations. In: Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA, Lippincott Williams & Wilkins; 2011:279.) |
 FIGURE 1.3 The ankle joint is completely surrounded by a dense capsule that provides support to the joint. Most of the strength of the ankle joint is provided by the deltoid, anterior talofibular, calcaneofibular, and posterior talofibular ligaments. (From Patel A, Horton G. Anatomy of the foot and ankle. In: Altcheck DW, DiGiovanni CW, eds. Foot and Ankle Sports Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:1–10.) |
Patients with ankle joint pain secondary to arthritis and collagen vascular disease related joint pain complain of pain that is localized to the ankle joint and distal lower extremity.
Activity, especially involving dorsiflexion of the ankle joint makes the pain worse, with rest and heat providing some relief. The pain is constant and characterized as aching. Sleep disturbance is common with awakening when the patient rolls over onto the affected ankle. Some patients complain of a grating, catching, or popping sensation with range of motion of the joint, and crepitus may be appreciated on physical examination.
Activity, especially involving dorsiflexion of the ankle joint makes the pain worse, with rest and heat providing some relief. The pain is constant and characterized as aching. Sleep disturbance is common with awakening when the patient rolls over onto the affected ankle. Some patients complain of a grating, catching, or popping sensation with range of motion of the joint, and crepitus may be appreciated on physical examination.
 FIGURE 1.4 Osteochondral defect (arrow) at the ankle. (From Eisenberg R. Clinical Imaging: An Atlas of Differential Diagnosis. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:1057.) |
 FIGURE 1.5 Synovial osteochondromatosis of the ankle. (From Eisenberg R. Clinical Imaging: An Atlas of Differential Diagnosis. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:1057.) |
 FIGURE 1.6 Lateral radiograph demonstrating joint mice which are causing ankle pain. |
Functional disability often accompanies the pain associated with many pathologic conditions of the ankle joint. Patients will often notice increasing difficulty in performing their activities of daily living and tasks that require walking, climbing stairs, and walking on uneven surfaces are particularly problematic. If the pathologic process responsible for the patient’s pain symptomatology is not adequately treated, the patient’s functional disability may worsen and muscle wasting may occur.
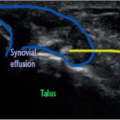
Plain radiographs are indicated in all patients who present with ankle pain as not only intrinsic ankle disease as well as other regional pathology may be perceived as ankle pain by the patient (Fig. 1.6). Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI, CT, or ultrasound of the ankle joint is indicated if the diagnosis is unclear as well as to identify other coexistent pathology (Fig. 1.7).
Related posts:
 Arthritis and Other Abnormalities of the Subtalar Joint
Arthritis and Other Abnormalities of the Subtalar Joint
 Arthritis and Other Abnormalities of the Talonavicular Joint
Arthritis and Other Abnormalities of the Talonavicular Joint
 Peroneal Tendinitis and Other Abnormalities of the Peroneus Longus and Brevis Tendons
Peroneal Tendinitis and Other Abnormalities of the Peroneus Longus and Brevis Tendons
 Calcaneal Spurs
Calcaneal Spurs
 Hallux Valgus Deformity
Hallux Valgus Deformity
 Plantar Fasciitis and Other Abnormalities of the Plantar Fascia
Plantar Fasciitis and Other Abnormalities of the Plantar Fascia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


