Peroneal Tendinitis and Other Abnormalities of the Peroneus Longus and Brevis Tendons
Anatomic Considerations
The peroneus longus and brevis muscles lie within the lateral peroneal compartment and function to help stabilize the ankle as well as plantarflex the foot at the ankle and evert the foot at the subtalar and transverse tarsal joints (Fig. 8.1). The peroneus longus muscle (which is also known as the fibularis longus muscle) finds its origin on the head and upper body of the fibula as well as the intermuscular septum and inserts via a strong tendon on the plantar side of the cuneiform bone and the first metatarsal (Fig. 8.2). The distal tendon of the peroneus longus muscle passes behind the lateral malleolus, lying within a groove along with the distal tendon of the peroneus brevis muscle (Fig. 8.3). The distal tendon of the peroneus longus muscle then passes beneath the superior fibular retinaculum extending obliquely across the lateral aspect of the calcaneus below the peroneal tubercle (which is also known as the trochlear process of the calcaneus) and inferior to the distal tendon of the peroneus brevis muscle. Crossing the lateral aspect of the cuneiform bone, the tendon then passes beneath peroneus brevis tendon and the cuneiform within a groove to pass obliquely across the sole of the foot to insert into the lateral aspect of the first metatarsal and the lateral side of the medial cuneiform bone (Figs. 8.4 and 8.5). It is at the two points where the tendon changes direction that it is most susceptible to the development of tendinitis.
The peroneus brevis muscle (which is also known as the fibularis brevis muscle) finds its origin more distally on the fibula and inserts at the tuberosity of the fifth metatarsal (Fig. 8.2). The muscle then passes inferiorly in front of and along with the peroneus longus muscle, with the distal tendon of the peroneus brevis muscle passing behind the lateral malleolus to run above the peroneal tubercle on the lateral side of the calcaneus to insert into the lateral side of the base of the fifth metatarsal bone (Figs. 8.3 to 8.5). Both peroneal muscles are supplied by the peroneal nerve.
Clinical Correlates
Peroneal tendinitis is a clinical syndrome characterized by sharp, constant, and severe ankle pain that is localized behind and just distal to the lateral malleolus. This painful condition is often seen as a result of acute inversion injuries to the ankle although it is also seen with overuse or misuse of the ankle and foot, as seen with repeated jumping and side-to-side movements required when playing soccer, basketball, and football. The problem is also seen in long distance running with improper shoes or from running on soft or uneven surfaces. The pain of peroneal tendinitis will be exacerbated with loading of the foot, especially with toe walking. With injury to the superior peroneal retinaculum, the tendons of both muscles may sublux creating additional ankle instability and a snapping sensation. With rupture of the tendons, pain and decreased strength is noted, especially with lateral cutting movements and push off portion of walking. If the acute insult to the tendons does not heal, the pain and functional disability can become chronic, with the pain waxing and waning depending on the patient’s level of activity.
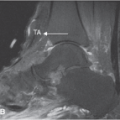
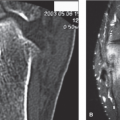
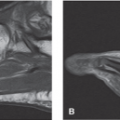
Patients suffering from peroneal tendinitis will often splint the inflamed peroneal tendon by adopting an antalgic gait to avoid using the affected tendon. This dysfunctional gait may cause a secondary bursitis and tendinitis around the foot and ankle which may serve to confuse the clinical picture and further increase the patient’s pain and disability. Pain on palpation of the peroneal tendon as it passes behind the lateral malleolus is a consistent finding in patients with peroneal tendinitis as is exacerbation of pain with active resisted eversion and toe walking (Fig. 8.6). The lateral aspect of the ankle may feel hot and appear swollen, which may be misdiagnosed as superficial thrombophlebitis or cellulitis. Patients suffering from peroneal tendinitis will also often complain that it feels like their shoes are rubbing the outside of their ankles raw, although on examination the skin appears normal. A creaking or grating sensation may be palpated when passively everting and inverting the ankle. Untreated, peroneal tendinitis will result in increasing pain, functional disability and calcium deposition around the tendon, which makes subsequent treatment more difficult. Continued trauma to the inflamed tendon ultimately may result in tendon tears and rupture (Figs. 8.7 to 8.9). Rupture of the peroneal tendon will result if disruption of the normal architecture of the tendon leads to alteration of the patient’s gait.
Plain radiographs are indicated in all patients who present with lateral ankle pain and foot pain. In the presence
of trauma, a careful search for a Jones fracture of the base of the fifth metatarsal is indicated (Fig. 8.10). Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI and/or ultrasound imaging of the ankle is indicated if peroneal tendinitis, rupture, fracture, or joint instability is suggested. Radionuclide bone scanning is useful to identify stress fractures of the bones of the ankle not seen on plain radiographs.
of trauma, a careful search for a Jones fracture of the base of the fifth metatarsal is indicated (Fig. 8.10). Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI and/or ultrasound imaging of the ankle is indicated if peroneal tendinitis, rupture, fracture, or joint instability is suggested. Radionuclide bone scanning is useful to identify stress fractures of the bones of the ankle not seen on plain radiographs.
 FIGURE 8.1 The anatomy of the peroneus longus and brevis muscles. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:122.) |
 FIGURE 8.2 The peroneus longus muscle (which is also known as the fibularis longus muscle) finds its origin on the head and upper body of the fibula as well as the intermuscular septum and inserts via a strong tendon on the plantar side of the cuneiform bone and the first metatarsal. The peroneus brevis muscle (which is also known as the fibularis brevis muscle) finds its origin more distally on the fibula and inserts at the tuberosity of the fifth metatarsal. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:116.) |
 FIGURE 8.3 The peroneus longus and brevis tendons are susceptible to the development of tendinitis as they pass behind the lateral malleolus. The peroneus longus tendon is also suceptible to the development of tendinitis at the point where it turns medially to pass beneath the peroneus brevis tendon. |
 FIGURE 8.4 The peroneus longus and brevis tendons. |
 FIGURE 8.5 The distal tendon of the peroneus longus muscle passes beneath the superior fibular retinaculum extending obliquely across the lateral aspect of the calcaneus inferior to the distal tendon of the peroneus brevis muscle. Crossing the lateral aspect of the cuneiform bone, the tendon then passes beneath the cuneiform within a groove to pass obliquely across the sole of the foot to insert into the lateral aspect of the first metatarsal and the lateral side of the medial cuneiform bone. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:138.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|