Achilles Tendinitis and Other Abnormalities of the Achilles Tendon
Anatomic Considerations
The Achilles tendon is the thickest and strongest tendon in the body, yet is also very susceptible to rupture. The common tendon of the gastrocnemius muscle, the Achilles tendon, begins at mid-calf and continues downward to attach to the posterior calcaneus, where it may become inflamed (Fig. 14.1). The Achilles tendon narrows during this downward course, becoming most narrow at approximately 5 cm above its calcaneal insertion. It is at this narrowest point that tendinitis also may occur (Fig. 14.2). A bursa is located between the Achilles tendon and the base of the tibia and the upper posterior calcaneus (see Fig. 14.2). This bursa also may become inflamed as a result of coexistent Achilles tendinitis and may confuse the clinical picture.
Clinical Correlates
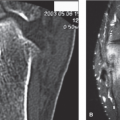
Achilles tendinitis is a clinical syndrome characterized by sharp, constant, and severe posterior ankle pain on plantar flexion of the ankle. Patients suffering from Achilles tendinitis will often splint the inflamed Achilles tendon by adopting a flat-footed gait to avoid plantar flexing the affected tendon. This dysfunctional gait may cause a secondary bursitis and tendinitis around the foot and ankle, which may serve to confuse the clinical picture and further increase the patient’s pain and disability. Pain on palpation of the insertion of the Achilles tendon on the calcaneus or at a point approximately 5 cm above the calcaneus at the narrowest part of the Achilles tendon is a consistent finding in patients with Achilles tendinitis as is exacerbation of pain with active resisted plantar flexion. Patients suffering from Achilles tendinitis will also exhibit a positive creaking tendon test. This test is performed by having the patient sit on the edge of the examination table. The examiner then palpates the Achilles tendon while passively plantar flexing and dorsiflexing the ankle (Fig. 14.3). The test is positive if the examiner appreciates a creaking sensation. Untreated, Achilles tendinitis will result in increasing pain and functional disability, calcium deposition around the tendon occurs, making subsequent treatment more difficult (Fig. 14.4). Continued trauma to the inflamed tendon ultimately may result in tendon rupture (Fig. 14.5).
The onset of Achilles tendinitis usually is acute, occurring after overuse or misuse of the ankle joint. Inciting factors may include activities such as running and sudden stopping and starting, as when playing tennis. Improper stretching of the gastrocnemius and Achilles tendon before exercise as well as the use of quinolone antibiotics have also been implicated in the development of Achilles tendinitis, as well as acute tendon rupture.
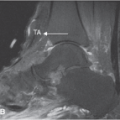
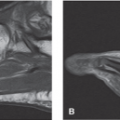
Plain radiographs are indicated in all patients who present with posterior ankle pain (Figs. 14.6 and 14.7). Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI and/or ultrasound imaging of the ankle is indicated if Achilles tendinitis, rupture, joint instability is suggested or the diagnosis is in question (Figs. 14.8 to 14.10). Radionuclide bone scanning is useful to identify stress fractures of the tibia not seen on plain radiographs.
Ultrasound Technique
To perform ultrasound evaluation of the Achilles tendon the patient is laced in the prone position with the patient’s ankle hanging off the edge of the table. With the patient in the above position, a high-frequency linear ultrasound transducer is placed in the longitudinal plane with the inferior portion of the ultrasound transducer over the insertion of the Achilles tendon on the calcaneus and an ultrasound survey scan is taken (Fig. 14.11). The linear Achilles tendon is identified as its insertion on the calcaneus (Fig. 14.12). When the insertion of the Achilles tendon is identified, the tendon is evaluated as the transducer is slowly moved in a cephalad direction while searching for fluid, extrinsic compression, tendinosis, tendinitis, tears, and rupture (Figs. 14.13 to 14.29). Ultrasound imaging of the Achilles tendon is also useful in identifying xanthomas associated with familial hypercholesterolemia. Color Doppler may aid in the identification of inflammation and the neovascularity associated with acute tears of the tendon and musculotendinous junction (Figs. 14.30 to 14.33).
Clinical Pearls
Bursitis and tendinitis of the ankle and foot may coexist with Achilles tendinitis and may contribute to the patient’s pain
symptoms. Early identification of pathology associated with tendinopathy of the Achilles tendon is crucial to avoid tendon rupture (Fig. 14.34). Ultrasound evaluation is also useful in assessment of healing of surgically repaired tears and ruptures of the Achilles tendon (Fig. 14.35). It is also important to identify the plantaris tendon which lies medial to the Achilles tendon and can sometimes be confused for residual Achilles tendon in the setting of complete Achilles tendon rupture (Fig. 14.36). Recent clinical experience has suggested that injection of platelet-rich plasma may be beneficial in patients with Achilles tendinosis to promote healing (Fig. 14.37).
symptoms. Early identification of pathology associated with tendinopathy of the Achilles tendon is crucial to avoid tendon rupture (Fig. 14.34). Ultrasound evaluation is also useful in assessment of healing of surgically repaired tears and ruptures of the Achilles tendon (Fig. 14.35). It is also important to identify the plantaris tendon which lies medial to the Achilles tendon and can sometimes be confused for residual Achilles tendon in the setting of complete Achilles tendon rupture (Fig. 14.36). Recent clinical experience has suggested that injection of platelet-rich plasma may be beneficial in patients with Achilles tendinosis to promote healing (Fig. 14.37).
 FIGURE 14.1 The common tendon of the gastrocnemius muscle, the Achilles tendon, begins at mid-calf and continues downward to attach to the posterior calcaneus, where it may become inflamed. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:117.) |
 FIGURE 14.2 The Achilles tendon is susceptible to the development of tendinitis at its insertion on the calcaneus as well at its narrowest point approximately 5 cm above the calcaneal insertion.
Related posts: Arthritis and Other Abnormalities of the Subtalar Joint Arthritis and Other Abnormalities of the Subtalar Joint
 Arthritis and Other Abnormalities of the Ankle Joint Arthritis and Other Abnormalities of the Ankle Joint
 Anterior Tarsal Tunnel Syndrome and Other Abnormalities of the Deep Peroneal Nerve Anterior Tarsal Tunnel Syndrome and Other Abnormalities of the Deep Peroneal Nerve
 Retrocalcaneal and Achilles Bursitis Retrocalcaneal and Achilles Bursitis
 Calcaneal Spurs Calcaneal Spurs
 Plantar Fasciitis and Other Abnormalities of the Plantar Fascia Plantar Fasciitis and Other Abnormalities of the Plantar Fascia
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|