CHAPTER 93 Acute Aortic Syndrome
Acute aortic syndrome describes a variety of potentially life-threatening aortic pathologic processes. These lesions include aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, aortic aneurysm leak and rupture, and traumatic aortic transection.1,2 The clinical presentation is often characterized by acute chest pain in patients with a history of hypertension. Chest pain is variously described as severe, tearing, or migratory. Symptoms can sometimes be confused with acute myocardial infarction or pulmonary embolism. Furthermore, the various types of acute aortic syndromes cannot be reliably differentiated by their clinical presentations.
Acute aortic syndrome is a clinical emergency. Accurate diagnosis and rapid treatment are essential to improve prognosis. Therefore, the aorta must be fully assessed by imaging when the syndrome is suspected. During the last 20 years, new imaging modalities have been developed that dramatically improve assessment of aortic disease. Computed tomography (CT), magnetic resonance imaging (MRI), and ultrasonography allow examination of aortic disease, providing more detail than that of chest radiography or catheter angiography.3
AORTIC DISSECTION
Prevalence and Epidemiology
Aortic dissection is the most common form of acute aortic syndrome. Incidence in the general population is reported from 2.9 to 3.5 cases per 100,000 person-years.4,5 Two thirds of patients are male. In women, aortic dissection typically presents at an older age (67 years versus 63 years in men).6
Etiology and Pathophysiology
The pathology of aortic dissection is a primary intimal tear that allows blood to enter the aortic media, extending proximally and distally into the aortic wall and displacing the intima inward. This entry tear typically occurs at sites of greatest wall tension, notably within a few centimeters of the aortic valve or close to the attachment site of the ligamentum arteriosum.2,7 The intima and inner part of the aortic media form the intimomedial flap, and the outer part of the aortic media and adventitia form the outer boundary of the false lumen (also known as a false channel; Fig. 93-1). The true lumen is directly connected to the lumen of the unaffected aorta and usually experiences high-velocity flow. The false lumen communicates with the true lumen through the intimal tear and experiences slower, turbulent blood flow. Re-entry tears are usually present in the intima, creating additional communication between the true and false lumens in the distal aorta.2
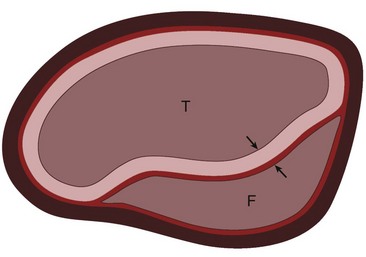
 FIGURE 93-1
FIGURE 93-1Most patients with aortic dissection have a history of systemic hypertension, which adds to the mechanical strains and shearing forces along the aortic wall. Long-standing hypertension is also associated with increased stiffness of the aortic media, which may introduce additional interlaminar shearing stresses and further contribute to the development of aortic dissection.2
Atherosclerotic disease may also be associated with aortic dissection, namely, through the development of a penetrating atherosclerotic ulcer. However, atherosclerosis is not a typical cause of aortic dissection. Dissection in patients with severe atherosclerosis tends to be limited by fibrosis and calcification, but the relationship between an atheroma and the location of aortic dissection is not clear in most patients.8 Other predisposing factors for aortic dissection include connective tissue disorders such as Marfan syndrome, Ehlers-Danlos syndrome, bicuspid aortic valve, aortitis, and aortic coarctation. Aortic dissection can also be caused iatrogenically by aortic surgery or percutaneous procedures such as catheterization and placement of intra-aortic balloon pumps.9,10
Manifestations of Disease
Clinical Presentation
Aortic dissection often presents as excruciating chest pain in a patient with a history of hypertension. The pain is usually described as severely intense, acute, searing or tearing, throbbing, and occasionally migratory. Involvement of the ascending aorta can cause anterior chest, neck, throat, and even jaw pain, whereas involvement of the descending aorta may cause back and abdominal pain.11 Ischemic symptoms usually are due to obstruction of the aortic branches by the dissection flap.
Aortic dissection is divided into acute and chronic forms according to the duration of symptoms. An acute form refers to dissection when the diagnosis is made within 2 weeks of symptom onset; in a chronic form, symptoms persist for more than 2 weeks. More than 60% of dissection-related mortality occurs in the first week of disease evolution and 74% within 2 weeks.12
Two classifications of aortic dissection are widely used according to the location and extent of involvement of the thoracic aorta. The DeBakey classification system uses three types (Fig. 93-2).13 Type I dissection involves the ascending aorta, the arch, and a variable length of the descending thoracic and abdominal aorta. Type II dissection is confined to the ascending aorta, and type III dissection may be confined to the descending thoracic aorta (type IIIa) or extend into the abdominal aorta and iliac arteries (type IIIb). The Stanford classification system divides aortic dissection into two types (see Fig. 93-2).14 Type A involves the ascending aorta, with or without involvement of the arch or the descending thoracic aorta. Type B dissection involves the descending thoracic aorta distal to the origin of the left subclavian artery.

 FIGURE 93-2 The two most widely used classifications of aortic dissection. The DeBakey classification includes three types.14 Type I: the intimal tear usually originates in the proximal ascending aorta; the dissection propagates to the aortic arch and often beyond it distally. Type II: the dissection originates in and is confined to the ascending aorta. Type III: the dissection originates in the descending thoracic aorta (type IIIa) or extends distally down the aorta and iliac arteries (type IIIb); the dissection rarely extends proximally into the aortic arch and ascending aorta. The Stanford classification has two types.15 Type A: dissection involves the ascending aorta, with or without involvement of the aortic arch or the descending aorta. Type B: dissection does not involve the ascending aorta.
FIGURE 93-2 The two most widely used classifications of aortic dissection. The DeBakey classification includes three types.14 Type I: the intimal tear usually originates in the proximal ascending aorta; the dissection propagates to the aortic arch and often beyond it distally. Type II: the dissection originates in and is confined to the ascending aorta. Type III: the dissection originates in the descending thoracic aorta (type IIIa) or extends distally down the aorta and iliac arteries (type IIIb); the dissection rarely extends proximally into the aortic arch and ascending aorta. The Stanford classification has two types.15 Type A: dissection involves the ascending aorta, with or without involvement of the aortic arch or the descending aorta. Type B: dissection does not involve the ascending aorta.
Imaging Indications and Algorithm
Diagnostic imaging is essential for proper evaluation of patients with suspected aortic dissection. The primary goals of imaging are to depict the intimal flap and to delineate the extent of aortic involvement and extension into the arch vessels and coronary arteries. It is also important to recognize associated complications, including pericardial hemorrhage, which can lead to life-threatening cardiac tamponade, periaortic or mediastinal hematoma, and pleural hemorrhage.15
Imaging techniques for dissection, consisting primarily of radiography and catheter angiography in the past, have changed rapidly in recent years. Multidetector CT (MDCT) and, to a lesser extent, ultrasonography and MRI have taken precedence and relegated catheter angiography to the occasional instance in which noninvasive imaging is not definitive or therapeutic intervention is desired.15 A meta-analysis found the diagnostic accuracy of CT, transesophageal echocardiography, and MRI to be virtually the same (95% to 100%) for the diagnosis of thoracic aortic dissection.16
Imaging Techniques and Findings
Radiography
Chest radiography is commonly performed as an initial study in patients with chest pain but is less sensitive for the diagnosis of aortic dissection. Chest radiography, however, does remain important because it may suggest an underlying aortic pathologic process, and it is performed routinely in patients with suspected aortic disease.15 The most common chest radiographic findings in patients with aortic dissection are widening of the mediastinum and aortic contour, disparity in the size of the ascending and descending aorta, changes in aortic configuration on serial studies, and displacement of a calcified plaque by more than 10 mm (Fig. 93-3).17 Other findings may include tracheal deviation, inferior displacement of the left main bronchus and opacification of the aorta-pulmonary window, and widening of the left paraspinal line.
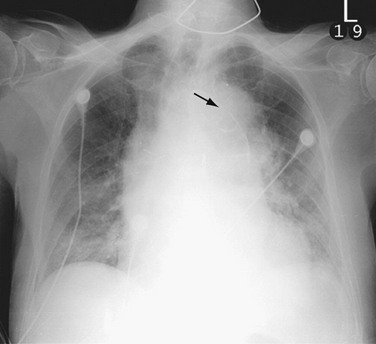
 FIGURE 93-3
FIGURE 93-3In practice, mediastinal widening is often difficult to evaluate on initial chest radiographs because patients are often examined in the supine position with portable radiography and are unable to hold the breath in full inspiration. Individual features suggestive of aortic dissection, such as displacement of aortic calcification, may be misdiagnosed because of the variable positions of the calcified plaque and the lateral aortic border.17 Proximal dissection is especially difficult to diagnose on chest radiographs. Serial studies can be helpful in identifying the changes between the prior and current studies.
Ultrasonography
Ultrasound techniques available for evaluation of aortic dissection include transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and intravascular ultrasound (IVUS).15 TTE is readily available, noninvasive, and portable but limited by a narrow acoustic window. It can be useful for evaluation of the aortic root, including aortic valve complications or cardiac and aortic wall motion abnormalities. TEE is a relatively invasive diagnostic procedure, but it can be performed at bedside and demonstrate true and false lumens, direction of blood flow, and complications such as aortic regurgitation on Doppler examination (Fig. 93-4). TEE typically provides broader and more accurate aortic visualization than does TTE for improved evaluation for aortic dissection; however, TEE cannot image the distal ascending aorta and proximal aortic arch completely as the airway may be positioned between the esophagus and the aorta.18 Catheter-based IVUS can provide imaging of the entire aorta with high sensitivity and specificity. However, it is limited in detecting the site of intimal tear, particularly in the ascending aorta.19 IVUS is rarely used in the initial screening or follow-up of patients with aortic dissection.
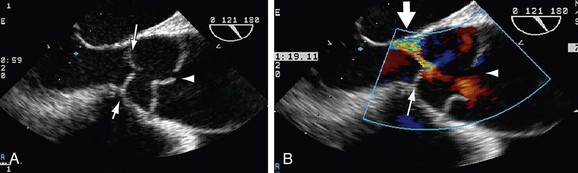
 FIGURE 93-4
FIGURE 93-4Diagnosis of aortic dissection by ultrasound examination requires demonstration of the true and false lumens separated by an intimal flap. To determine the therapeutic implications, one must evaluate the involvement of the ascending aorta, the coexistence of aortic insufficiency, the site of the original tear, the characteristics of blood flow and clot formation in the false lumen, the relative position of the coronary arteries, and the involvement of the aortic arch vessels, notably the carotid arteries. Ventricular function and the presence of pericardial effusion are also important for therapeutic strategy.3
The advantage of ultrasonography over MRI or CT is its portability, which makes it useful at the bedside or in the operating room. However, objective and reproducible thoracic aortic evaluation with ultrasonography remains problematic given operator dependence and restricted thoracic acoustic windows. Ultrasonography, moreover, is prone to artifacts and the detection of “pseudolesions,” such as reverberation artifacts, which can be misdiagnosed as aortic dissection and cause false-positive study results.15
Computed Tomography
CT is the most commonly used diagnostic tool in patients with suspected aortic dissection. A study from the International Registry of Acute Aortic Dissection reported that CT was used in 61% of cases as the primary diagnostic procedure for detection of aortic dissection. Ultrasonography was used in 33% of cases, followed by catheter angiography in 4.4% and MRI in 1.8%.6 The advantages of CT scans are faster scanning, high spatial resolution, and the ability with moving table bolus chase imaging to provide extended anatomic coverage for illustration of the entire thoracoabdominal aorta. The development of multidetector technology has allowed acquisition of submillimeter-thick axial images, which can provide isotropic imaging volumes for improved postprocessed viewing of complex arterial geometries and relationships. Compared with ultrasonography, MDCT benefits from being less operator dependent, having a relative ease of use, and providing a larger field of view for improved detection of both vascular and extravascular findings. The key disadvantages of MDCT include its use of ionizing radiation and iodine-based intravenous contrast agents, which are contraindicated in certain patients.15
CT is highly accurate, with a sensitivity and a specificity of more than 95% reported for the diagnosis of aortic dissection.3 Compared with ultrasonography and MRI, CT also provides an improved ability to evaluate for confounding differential diagnoses in the thorax and abdomen (Fig. 93-5).
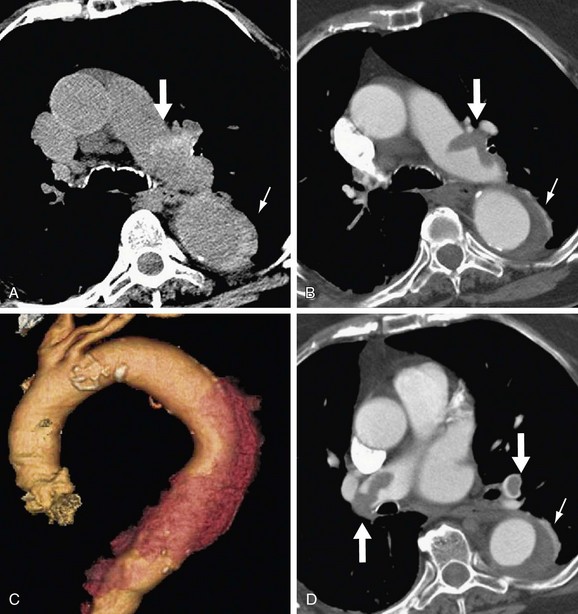
 FIGURE 93-5
FIGURE 93-5Although major diagnostic clues are provided by contrast-enhanced CT scans, the importance of non–contrast-enhanced scans should not be overlooked. Non–contrast-enhanced CT scans can depict intimal calcifications and high-density lesions from leaking or thrombosed blood in the aortic wall, in periaortic regions, or in pleural and pericardial spaces.20
The main CT findings in aortic dissection include variable appearances of the true and false lumens, involvement of the ascending aorta, extension into arterial branches, and associated lesions.15,21,22 The intimal flap divides the aortic lumen into two channels, and the true lumen is typically more opacified than the false lumen because of the higher blood pressure and faster mixing of blood with contrast material in the true lumen on early arterial phase images (Fig. 93-6). True and false lumens can be differentiated on the basis of other characteristics. The true lumen is generally posterior and left posterolateral in the ascending aorta, caudal in the aortic arch, and anterior and right anterolateral in the descending aorta. The true lumen tends to be smaller than the false lumen because of inward displacement of the intimal flap. Thrombus is commonly found in the false lumen because of its slow flow. Multiphase contrast-enhanced CT scans may show that the false lumen enhances later and washes out in a delayed fashion.21
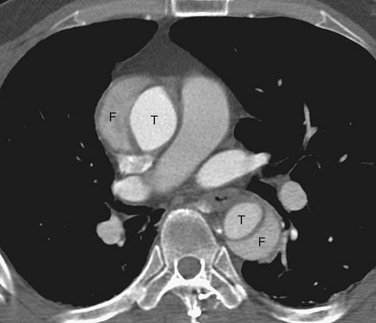
 FIGURE 93-6
FIGURE 93-6Demonstration of the intimal flap on CT images is accurate and precise in the descending aorta. In contrast, the dissecting flap in the ascending aorta can be difficult to properly identify as it may be confused with aortic valve cusps on axial images or mistaken for motion artifacts of the aortic root due to cardiac or respiratory movement (Fig. 93-7). However, these artifacts can be minimized by use of a rapid scan technique and cardiac synchronization (i.e., either prospective ECG triggering or retrospective ECG gating).23
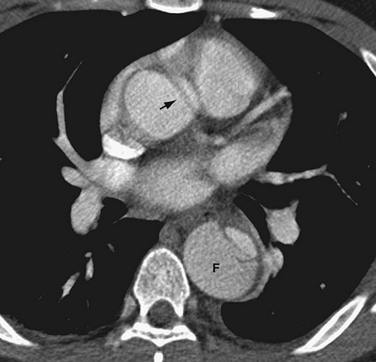
 FIGURE 93-7 Type B aortic dissection in which the false lumen (F) is noted on non–ECG-gated, contrast-enhanced CT to be larger than the true lumen in the descending thoracic aorta. An artifactual dark linear band (arrow) mimics an intimal tear in the ascending aorta. This artifact is secondary to through-plane motion of the geometrically complex and obliquely positioned aortic root and can be minimized by ECG-gated CT acquisition. Note that genuine intimal tears are more typically oriented in the right anterolateral aspect of the ascending aorta (see Fig. 93-6).
FIGURE 93-7 Type B aortic dissection in which the false lumen (F) is noted on non–ECG-gated, contrast-enhanced CT to be larger than the true lumen in the descending thoracic aorta. An artifactual dark linear band (arrow) mimics an intimal tear in the ascending aorta. This artifact is secondary to through-plane motion of the geometrically complex and obliquely positioned aortic root and can be minimized by ECG-gated CT acquisition. Note that genuine intimal tears are more typically oriented in the right anterolateral aspect of the ascending aorta (see Fig. 93-6).
Magnetic Resonance
Like CT, MRI has been reported to have a sensitivity and specificity of more than 95%3; thus, it is a suitable alternative to catheter angiography for the diagnosis and evaluation of aortic dissection. T1- and T2-weighted black blood spin-echo MR images provide high tissue contrast between the blood pool, the vascular wall, and the adjacent soft tissues. Cine bright blood imaging provides supplemental images for improved detection of the intimal flap and extent of the true and false lumens as well as functional information about blood flow associated with the aortic dissection. Moreover, cine MR enables evaluation of the aortic valve and its function.16
On black blood spin-echo images, the true and false lumens are depicted as regions of signal void, and the intimal flap is seen as a linear structure of isointense signal intensity that is outlined by the flow void in the dual lumens (Fig. 93-8). The false lumen can be differentiated from the true because the flow is slower and thrombus is more likely to form. If the false lumen contains thrombus, the intimal flap may not be seen because it is not outlined by moving blood on both sides. Although MRI is superior to CT in depicting the presence of blood flow, non–contrast-enhanced MRI is sometimes unable to differentiate slowly moving blood from thrombus in the false lumen.17
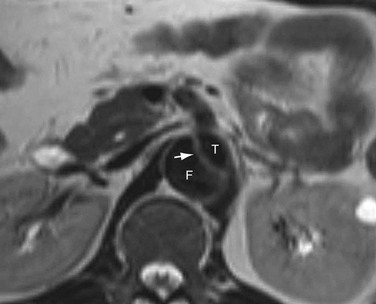
 FIGURE 93-8
FIGURE 93-8Aortic MR angiography (MRA) can be performed with time-of-flight and phase contrast techniques.24,25 These flow-based techniques may be helpful in differentiating the signal intensities between slow blood flow and intravascular thrombus. However, the disadvantage of these techniques is relatively long scan time, which restricts their use in hemodynamically unstable patients.
Aortic MRA is more routinely performed with use of gadolinium-enhanced three-dimensional MRA.26 Gadolinium-enhanced MRA has dramatically shortened total examination time in the diagnosis of aortic dissection and has replaced non–contrast-enhanced MRA techniques. Like contrast-enhanced CT angiography (CTA), gadolinium-enhanced MR provides arterial “luminograms” that can be postprocessed by an array of three-dimensional processing tools on an independent workstation. The advantages of gadolinium-enhanced MRA over contrast-enhanced CTA include its use of generally safer gadolinium-chelate contrast agents, lack of ionizing radiation, and production of high contrast images with fewer image sections. Furthermore, postprocessing is much faster with gadolinium-enhanced MRA than with CTA.27 Like contrast-enhanced CTA, gadolinium-enhanced MRA can differentiate the true and false lumens according to their signal intensity differences (Fig. 93-9). The intimal flap is visualized as a line of low signal intensity with a linear or curved shape. The true lumen often has higher signal intensity than the false because of a higher concentration of contrast material during the arterial phase. The acquisition of delayed images improves depiction of thrombosis of the false lumen, which can be easily depicted as lower signal intensity.

 FIGURE 93-9
FIGURE 93-9Despite these advantages of MR techniques, MRI is rarely used as the initial imaging modality for the evaluation of aortic dissection. Data from the International Registry of Acute Aortic Dissection revealed that only 1.8% of patients with aortic dissection underwent MRI as an initial imaging test, which was less often than catheter aortography (4.4%).6 This may be due to limited emergent availability of MRI, incompatibility with implanted metal devices such as pacemakers and aneurysm clips, or monitoring difficulties during examination. Furthermore, MRI is not suitable in patients with hemodynamic instability. The use of MRI may also be restricted in patients with claustrophobia15 or with renal insufficiency, in whom there is an increased risk for development of nephrogenic systemic fibrosis after the intravenous administration of gadolinium-chelate contrast agents.
Angiography
Angiographic signs of aortic dissection can be categorized as direct or indirect. Direct findings include visualization of the intimal flap or dual lumens (Fig. 93-10). Indirect findings include compression of the true lumen, thickening of the aortic wall, abnormalities of branch vessels, and aortic insufficiency.17 The major advantage of catheter angiography is its ability to evaluate the aortic valve and extent of involvement of major aortic branches. Sensitivity and specificity of catheter angiography for diagnosis of dissection are 88% and 94%.28

 FIGURE 93-10
FIGURE 93-10Although catheter angiography is sensitive for the diagnosis of aortic dissection, it has recently been replaced by noninvasive modalities such as CT, ultrasonography, and MRI.29 Proper diagnosis of aortic dissection may be difficult in situations in which the false lumen is not opacified or in which both lumens are equally opacified. The false lumen may not be opacified when it is thrombosed, when there is no intimal tear, or when the catheter tip is distal to the site of the intimal tear.17 In addition, because catheter angiography cannot directly depict the aortic wall, it cannot accurately evaluate the size of the aorta, intramural features of the aortic wall, or periaortic complications. The higher false-negative rate, therefore, results from its inability to identify extraluminal abnormalities such as an intramural hematoma, thrombosed false lumens, and periaortic fluid collections. Because of its invasiveness and time-consuming nature, the use of catheter angiography in the diagnosis of aortic disease has been dramatically reduced.15
Classic Signs
On cross-sectional imaging, the “beak sign” can be seen at the corner of the false lumen, forming an acute angle with the intimomedial flap and the outer wall of the aorta (Fig. 93-11).30 The “cobweb sign” of the medial layer sometimes persists between the intima and media, forming thin strands of medial tissue that can be seen crossing the false lumen (Fig. 93-12).31
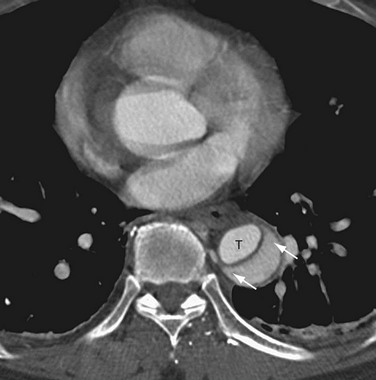
 FIGURE 93-11
FIGURE 93-11
 FIGURE 93-12
FIGURE 93-12Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


