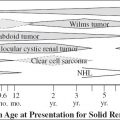
NHL > Burkitt lymphoma, Hodgkin disease
√ bilateral multiple renal masses:
√ slightly hyperattenuating relative to renal parenchyma on NECT
√ hypoattenuating homogeneous masses during nephrographic phase on CECT
√ direct extension of retroperitoneal lymphadenopathy engulfing kidney, renal sinus, ureter
5. Kaposi sarcoma (27%)
= AIDS-defining illness usually in patients with CD4 lymphocyte count < 150–200 cells/mm3
Histo: renal tissue replaced + infiltrated by proliferation of spindle cells with characteristic small vascular spaces + demonstrable nuclear staining for HHV8
√ renal enlargement + irregular hypoattenuating areas in renal cortex
6. HAART-related nephropathy
[highly active antiretroviral therapy]
• acute renal failure ← renal tubular damage from nucleotide reverse-transcriptase inhibitors (tenofovir, adefovir, cidofovir)
• dyslipidemia, insulin resistance, fat redistribution
• hypertension
√ renal calculi (in up to 20%) ← indinavir and nelfinavir
√ renal artery stenosis
7. Cystitis (22%)
Organism: routine gram-negative species, Candida, beta-hemolytic streptococci, Salmonella, CMV
√ bladder wall thickening
ACUTE CORTICAL NECROSIS
= rare form of acute renal failure
Etiology:
(a) ischemia ← vasospasm of small vessels
(b) toxic damage to glomerular capillary endothelium
(c) primary intravascular thrombosis
At risk:
(a) Obstetric patient (most often): abruptio placentae = premature separation of placenta with concealed hemorrhage (50%), septic abortion, placenta previa
(b) Children: severe dehydration + fever, infection, hemolytic uremic syndrome, transfusion reaction
(c) Adults: sepsis, severe dehydration, acute prolonged shock, myocardial failure, burns, venomous snakebite, abdominal aortic surgery, hyperacute renal transplant rejection
Histo: patchy / universal necrosis of renal cortex + proximal convoluted structures ← distension of glomerular capillaries with dehemoglobulinized RBCs; medulla and 1–2 mm of peripheral cortex are spared
• protracted + severe oliguria / anuria
Distribution: diffuse / multifocal; mostly bilateral
A. EARLY SIGNS
√ diffusely enlarged smooth kidneys
√ absent / faint nephrogram
CT:
√ enhancing interlobar and arcuate arteries adjacent to nonenhancing cortex (arterial phase)
√ “reversed rim” sign = enhancement of medulla + nonenhancement of hypoattenuating cortex (parenchymal phase)
Cause: sustained hypotension for 1 hour
√ rim of subcapsular cortical enhancement ← collateral blood flow from cortical vessels
√ enhancement of juxtamedullary zone of cortex
US:
√ loss of normal corticomedullary region with hypoechoic outer rim of cortex
NUC:
√ severely impaired renal perfusion
B. LATE SIGNS
√ small kidney (after a few months)
√ “tramline” / punctate calcifications along margins of viable and necrotic tissue (as early as 1–2 months)
US:
√ hyperechoic cortex with acoustic shadowing
Prognosis: poor chance of recovery
ACUTE INTERSTITIAL NEPHRITIS
= infiltration of interstitium by lymphocytes, plasma cells, eosinophils, few PMNs + edema
Cause: allergic / idiosyncratic reaction to drug exposure (penicillin, methicillin, sulfonamides, ampicillin, cephalotin, anticoagulants, phenindione, diphenylhydantoin)
• eosinophilia (develops 5 days to 5 weeks after exposure)
√ large smooth kidneys with thick parenchyma
√ normal / diminished contrast density
US:
√ normal / increased echogenicity
ACUTE TUBULAR NECROSIS
= ACUTE VASOMOTOR NEPHROPATHY
= temporary reversible marked reduction in tubular flow rate
Etiology:
(a) DRUGS: bichloride of mercury, ethylene glycol (antifreeze), carbon tetrachloride, bismuth, arsenic, uranium, urographic contrast material (esp. when associated with glomerulo-sclerosis in diabetes mellitus), aminoglycosides (gentamicin, kanamycin)
(b) ISCHEMIA: major trauma, massive hemorrhage, postpartum hemorrhage, crush injury, myoglobulinuria, compartmental syndrome, septic shock, cardiogenic shock, burns, transfusion reaction, severe dehydration, pancreatitis, gastroenteritis, renal transplantation, cardiac surgery, biliary surgery, aortic resection
Pathophysiology: profound reduction in renal blood flow ← elevated arteriolar resistance
√ smooth large kidneys, especially increase in AP diameter > 4.63 cm ← interstitial edema
√ diminished / absent opacification of collecting system
√ immediate persistent dense nephrogram (75%)
√ increasingly dense persistent nephrogram (25%)
√ diffuse calcifications (rare)
US:
√ normal to diminished echogenicity of medulla
√ sharp delineation of swollen pyramids
√ normal (89%) / increased (11%) echogenicity of cortex
√ elevated resistive index ≥ 0.75 (in 91% excluding patients with hepatorenal syndrome); unusual in prerenal azotemia
Angio:
√ normal arterial tree with delayed emptying of intrarenal vessels
√ slightly delayed / normal venous opacification
NUC:
√ well-maintained renal perfusion
√ poor concentration of 99mTc-glucoheptonate / 99mTc-DTPA
√ better renal visualization on immediate postinjection images than on delayed images
√ progressive parenchymal accumulation of 131I-Hippuran / 99mTc-MAG3
√ no excretion
ADDISON DISEASE
= PRIMARY ADRENAL INSUFFICIENCY
◊ 90% of adrenal cortex must be destroyed!
Course: acute (adrenal apoplexy), subacute (disease present for < 2 years), chronic
Acute Primary Adrenal Insufficiency
= ADDISONIAN CRISIS = ADRENAL APOPLEXY
Cause: bilateral adrenal hemorrhage most commonly due to stress from surgery / sepsis / hypotension with shock / hemorrhagic diathesis, anticoagulation therapy
• abdominal / back pain
• fever (70%), hyperpyrexia, lethargy, nausea, vomiting
√ bilateral adrenal enlargement with areas of increased attenuation
Cx: catastrophic hypotension + shock
Chronic Primary Adrenal Insufficiency
Cause:
1. Idiopathic adrenal atrophy (60–70%): likely autoimmune disorder
2. Fungal infection: histoplasmosis, blastomycosis, coccidioidomycosis
3. Granulomatous disease: tuberculosis, sarcoidosis
4. Bilateral metastatic disease (rare)
• hyponatremia, hyperkalemia, azotemia, hypercalcemia
√ diminutive glands ← idiopathic atrophy + chronic inflammation
√ calcifications (in 25% of chronic course)
ADENOMATOID TUMOR OF SCROTUM
= benign slow-growing mesothelial neoplasm
Frequency: 30% of all extratesticular masses;
2nd most common extratesticular mass (after lipoma)
Age: 2nd–4th decade
Histo: epithelial-like cells + stroma of hyalinized / loose collagen with varying amounts of smooth muscle + elastic fibers
Origin: epididymal tail
Location: epididymis > tunica vaginalis, spermatic cord (rare)
Site: L > R; lower pole÷upper pole = 4÷1
Size: 0.4–5.0 cm (usually < 2 cm)
• hard painless scrotal mass
√ smooth round paratesticular mass at periphery of testis:
√ well-marginated solid hypoechoic mass with echogenicity equal to / greater than testis
√ indentation of the testicular contour
MR:
√ isointense relative to testis on T1WI
√ slightly hypointense relative to testis on T2WI
√ enhancement similar to testicular enhancement
DDx: germ cell tumor, granulomatous epididymitis (painful, avascular), metastasis from B-cell ALL / NHL
ADRENAL CYST
Frequency: 0.06–0.18% (at autopsy)
Age: 3rd–5th decades (most commonly); M÷F = 1÷3 to 1÷2
| Path: | (a) | vascular / endothelial cyst (45–48%) |
| (b) | pseudocyst (39–42%) | |
| (c) | epithelial lining = true simple cyst (9–10%) | |
| (d) | parasitic cyst (7%) |
Location: mostly solitary; R÷L = 1÷1; bilateral in 8–15%
Mean size: 5.3 cm; < 5 cm in diameter in 50% (up to 20 cm)
• asymptomatic, unless very large / infected / ruptured / bled into
√ well-circumscribed encapsulated uni- / multilocular lesion with internal septa
√ thin wall of < 3 mm in thickness (unless pseudocyst)
√ lack of central enhancement ± wall and septal enhancement
√ calcifications:
(a) peripheral / mural: rimlike / nodular (51–69%)
(b) central (rarely): in intracystic septation (19%) / punctate within intracystic hemorrhage (5%)
(c) scattered throughout the lesion
Radiography:
√ inferior displacement of ipsilateral kidney
US:
√ well-circumscribed hypo- to anechoic lesion
CT:
√ well-circumscribed nonenhancing hypoattenuating lesion of < 20 HU (near-water density); higher attenuation with hemorrhage / intracystic debris / crystals
MR:
√ uniformly hypointense on T1WI + hyperintense on T2WI
√ NO enhancement
√ T1 hyperintense signal ← hemorrhage
√ ± septations / soft-tissue component ← hemorrhage / hyalinized thrombus
Cx: hypertension; hemorrhage; infection; rupture with retroperitoneal hemorrhage
Prognosis: interval increase in cyst size in 60%
| Rx: | (1) Resection of cyst > 5 cm ← risk of hemorrhage |
(2) Functional symptomatic cyst | |
(3) Cyst worrisome for malignancy |
DDx: (a) benign
1. Cystic pheochromocytoma
2. Cystic adenomatoid tumor
3. Schwannoma
4. Adrenocortical adenoma (contrast enhancement, no wall, no peripheral calcification)
5. Hemangioma
(b) benign
1. Cystic adrenocortical carcinoma (thick-walled lesion > 7 cm in size; extremely rare)
2. Metastatic disease
Vascular / Endothelial Adrenal Cyst (45–48%)
| Cause: | 1. | Simple cyst without soft-tissue component |
| 2. | Lymphangioma | |
| 3. | Hemangioma |
Histo: lined by cells resembling normal endothelium
√ multilocular thin-walled cyst containing serous / serosanguinous / clear fluid
√ scattered / central septal calcifications in 15–30%
Adrenal Pseudocyst (39–42%)
Cause:
1. Previous hemorrhage / infarction
2. Hemorrhagic complication of benign vascular neoplasm / malformation
3. Cystic degeneration / hemorrhage of primary adrenal mass
Histo: wall consists of dense hyalinized material + occasional calcification / osseous metaplasia; adrenal cortical cells can be found in wall
• amorphous material + blood products as content
√ typically unilocular thick-walled cyst > 3.5 mm
√ internal scattered echogenicity ← debris / fluid-fluid levels from recent hemorrhage
√ peripheral calcifications
True Simple / Epithelial Adrenal Cyst (9–10%)
| Cause: | 1. | Glandular / retention cyst |
| 2. | Embryonal cyst | |
| 3. | Cystic adenoma | |
| 4. | Mesothelial inclusion cyst |
Histo: simple epithelial lining
√ unilocular thin-walled cyst
Parasitic Adrenal Cyst (7%)
Cause: usually Echinococcus granulosus
Path: purely cystic to more complex contents depending on stage of infection
√ variable internal complexity ← daughter vesicles, freed scolices, brood capsules
√ septal / mural calcifications
√ “water lily” sign
√ extra-adrenal foci of hydatid disease
ADRENAL HEMORRHAGE
Site: medulla with variable degree of cortical involvement
• sudden / gradual onset of lower chest / upper abdominal / flank / back pain; shocklike symptoms = signs of massive blood loss
• acute adrenal insufficiency (rare): manifesting as hypotension + hyponatremia + hyperkalemia
√ round / oval mass displacing kidney inferiorly + IVC anteriorly
√ uniform adrenal enlargement gradually decreasing in size over 6–8 weeks (follow-up for 2–3 months)
√ complete resolution with time:
√ ± rimlike curvilinear / eggshell calcifications > 1 year
√ no enhancement
NECT:
@ acute stage (< 7 days):
√ round / oval mass (in 83%) located in medulla + stretching cortex around hematoma:
√ hyperattenuating (50–90 HU) similar to most neoplasms in acute stage → slowly decreasing over time
N.B.: Follow-up required to confirm regression!
√ obliteration of gland by diffuse irregular hemorrhage (in 9%)
√ periadrenal fat stranding
√ asymmetric thickening of diaphragmatic crus ← periadrenal hemorrhage
@ chronic stage (> 7 weeks):
√ mass with hypoattenuating center ± calcifications = adrenal pseudocyst (DDx: adrenal adenoma)
US (modality of choice for neonate):
√ complex solid heterogeneously hyperechoic mass during early stage
√ mixed echogenicity with centrally hypoechoic region (as liquefaction occurs)
√ peripheral curvilinear hyperechoic calcifications appearing within 1–2 weeks
√ completely anechoic / cystlike in chronic stage
√ avascularity on color Doppler / power Doppler
MR:
@ acute stage (< 7 days):
= high concentration of intracellular deoxyhemoglobin with preferential T2 proton relaxation enhancement
√ isointense / slightly hypointense on T1WI
√ markedly hypointense on T2WI
@ subacute stage (7 days–7 weeks):
= T1 shortening ← paramagnetic effect of free methemoglobin (Fe3+) ← produced by oxidation of hemoglobin (Fe2+)
√ hyperintensity on T1WI and T2WI appearing in periphery with filling in (over several weeks)
√ hematoma may be multilocular, each locule with its own different signal intensity
@ chronic stage (> 7 weeks):
= T2 proton relaxation enhancement ← hemosiderin deposition + presence of a fibrous capsule
√ hypointense rim on T1WI + T2WI
√ “blooming effect” (= magnetic susceptibility) of hemosiderin in gradient-echo imaging
Rx: supportive; prompt glucocorticoid administration with concomitant intravenous saline therapy for acute adrenal insufficiency
Nontraumatic Adrenal Hemorrhage (20%)
Incidence: in 1.8% (autopsy study)
| Cause: | (1) | Stress: severe burn, sepsis, surgery, hypotension |
| (2) | Hemorrhagic diathesis: anticoagulant therapy | |
| (3) | Coagulopathy | |
| (4) | Underlying adrenal mass: adrenocortical adenoma / carcinoma, myelolipoma, pheochromocytoma, metastasis, neuroblastoma |
Location: typically bilateral
DDx: neuroblastoma (stippled calcifications, increase in vanillylmandelic acid, no decrease on follow-up)
Blunt Trauma to Adrenal Gland (80%)
Incidence: in 28% of autopsies; in 2% of trauma CTs
◊ Adrenal injury means exposure to major force!
Mechanism:
(a) direct crush injury between spine and liver / spleen
(b) acutely increased adrenal venous pressure ← transmitted from compressed IVC / adrenal venous sampling
(c) IVC-adrenal vein thrombosis
(d) shear injury to small adrenal vessels (from rotational / deceleration forces)
Often associated with: injury to liver + kidney
Location: R÷L÷bilateral = 75÷15÷10
| Prognosis: | (1) | unilateral hematoma: spontaneous resolution without sequelae |
| (2) | bilateral hemorrhage: acute primary adrenal insufficiency (rare) is life-threatening |
DDx: preexisting adrenal mass → repeat imaging after 8–10 weeks!
ADRENOCORTICAL ADENOMA
◊ Most common tumor of adrenal gland!
Prevalence: 1–2% in general population; age-dependent 6.6–8.7% at autopsies (small tumors in 50% of autopsies)
◊ In a patient with lung carcinoma a solitary small adrenal mass is more likely an adenoma than a metastasis!
Path: atypical intralesional cystic degeneration / less often hemorrhage
Histo: clear cells arranged in cords with abundant intracellular (= intracytoplasmic) pale-staining lipid; rich delicate vascular network
◊ Detection of lipid by CT / MRI is NOT 100% specific!
DDx: metastatic clear cell renal cell carcinoma, pheochromocytoma, adrenocortical carcinoma
◊ No lipid may mean a benign lipid-free adenoma!
◊ Fat cell aggregates (macroscopic fat) may be present!
DDx: lipomatous / myelolipomatous metaplasia
• usually nonfunctioning
Average size: 2.0–2.5 cm: usually < 5 cm in size
√ well-defined homogeneous (87%) sharply marginated mass
√ small adenomas < 1 cm often go undetected
√ contralateral gland often normal / atrophic
NECT:
Categories:
(a) lipid-rich adenoma < 10 HU (60–90% of all adenomas)
(b) lipid-poor adenoma > 10 HU (up to 40%)
√ soft-tissue density / cystic density (mimicked by high cholesterol content) with poor correlation between functional status and HU number:
√ < 0 HU on NECT (47% sensitive, 100% specific)
√ < 10 HU on NECT (79% sensitive, 96% specific)
√ < 18 HU on NECT (85% sensitive, 100% specific)
√ > 10% negative pixels on histogram (100% specific)
√ homogeneous attenuation (87%)
CECT:
√ homogeneous (58%) enhancement
√ < 37 HU on 5–15-min delayed CECT is DIAGNOSTIC of adenoma
Washout Technique:
Rationale: adenomas show significantly more initial enhancement than nonadenomas
(1) Attenuation before contrast administration = ANECT
(2) Early attenuation at 60 sec = Aearly
(3) Delayed attenuation at 10–15 min = Adelayed
(4) Absolute percentage washout (Wabs / APW)
Wabs = [1 – (Adelayed –ANECT) / (Aearly – ANECT)] • 100
√ washout > 40% = adenoma
√ washout ≤ 40% = indeterminate mass
(5) Relative percentage washout (Wrel / RPW) useful when the NECT value is not known
Wrel = [(Aearly – Adelayed)/Aearly] • 100
√ washout > 60% = adenoma
√ washout ≤ 60% = indeterminate mass
Angio:
√ tumor blush + neovascularity; occasionally hypovascular
√ pooling of contrast material
√ enlarged central vein with high flow
√ arcuate displacement of intraadrenal veins
√ bilateral adrenal venous sampling → in up to 40% unsuccessful in localizing
MR:
√ isointense mass relative to liver + hyperintense relative to spleen on T1WI ← short T1 time of lipid
√ iso- / hypointense mass (rarely hyperintense) to spleen on T2WI
√ marked hypointensity compared with spleen / skeletal muscle on opposed-phase GRE images ← destructive interference of lipid and water signals = phase cancellation of fat + water protons in same voxel in 95% of adenomas (> 90% accurate)
√ signal loss of ≥ 20% on opposed-phase image
√ India ink effect = characteristic black lines outlining interface between organ + adjacent fat (chemical shift artifact)
√ small round foci of altered SI ← cystic changes / hemorrhage / variation in vascularity
CEMR:
√ uniform enhancement on immediate early imaging
√ adenomas tend to enhance less rapidly + less intensely than metastases on time-enhancement curves
√ relatively rapid washout of contrast material compared with metastases with return to baseline at 15 minutes ← lack of large interstitial spaces of edema + necrosis (DDx: metastases tend to have higher signal intensities [however 20–30% overlap])
US:
√ well-circumscribed round or oval lesion of slightly heterogeneous mixed echogenicity
Atypical appearance:
◊ Occasional intralesional cystic degeneration / hemorrhage make an accurate diagnosis more challenging!
√ adenoma may calcify → often in areas of old hemorrhage
DDx: pheochromocytoma, adrenocortical carcinoma, metastasis, functioning adenoma
Nonhyperfunctioning Adrenocortical Adenoma
characterized by
(a) normal lab values of adrenal hormones
(b) NO pituitary shutdown of the contralateral gland
(c) activity on NP-59 radionuclide scans
Prevalence: incidental finding in 0.6–1.5% of CT examinations, in 3–9% at autopsy
√ surveillance CT to confirm lack of growth
Rx: surgical removal for masses 3–5 cm as indeterminate potentially malignant neoplasms
DDx: metastasis
Hyperfunctioning Adrenocortical Adenoma
√ contralateral adrenal atrophy ← suppression of pituitary ACTH by elevated cortisol levels
1. Primary hyperaldosteronism = Conn syndrome (80%)
Pathophysiology: secretion of aldosterone by an adenoma is pulsatile
√ ACTH infusion incites a dramatic increase in levels of cortisol + aldosterone for venous sampling
2. Cushing syndrome (10%)
3. Virilization
(a) hirsutism + clitoromegaly in girls
(b) pseudopuberty in boys
◊ Most common type of hormone elevation in children!
• elevated testosterone levels > 0.55 ng/mL
4. Feminization (estrogen production)
√ contralateral atrophic gland ← ACTH suppression with autonomous adenoma
√ unilateral focus of 131I NP-59 radioactivity + contralateral absence of iodocholesterol accumulation (DDx: hyperplasia [bilateral activity])
ADRENOCORTICAL CARCINOMA
Prevalence: 1–2÷1,000,000 people; 0.3–0.4% of all pediatric neoplasms (3 x more likely than adrenal adenoma)
Age: biphasic distribution (1st + 4th–5th decade); M÷F = 1÷1.5
May be associated with:
hemihypertrophy, Li-Fraumeni syndrome, Beckwith-Wiedemann syndrome, Carney complex, congenital adrenal hyperplasia, MEN 1, astrocytomas
Path: large lobulated tumor, often with cystic / necrotic / hemorrhagic center
Histo: differentiation of benign from malignant solely on the basis of histologic features may be difficult
• abdominal / back pain, palpable abdominal mass
• weight loss, early satiety
• 20% nonfunctioning
• 50% hyperfunctioning (in 10–15% Cushing syndrome, occasionally Conn syndrome, feminization, adrenogenital syndrome with virilization) inversely related to size
• hypertension (common in all syndrome types)
Location: left÷right adrenal = 53÷47; bilateral in 10%
Median size: 10–12 cm (range, 4–25 cm); usually > 5 cm; in 70% > 6 cm in diameter
A heterogeneous enhancing adrenal mass > 4 cm in diameter has a high likelihood of malignancy!
√ frequently heterogeneous mass with irregular margins + displacement of regional structures
√ occasionally calcified (in 19–33%)
√ invasion of IVC, liver, kidney, diaphragm (multiplanar imaging helpful)
√ metastases to liver, regional lymph nodes, lung, bone, brain
◊ Metastases are the only reliable sign of malignancy!
◊ Large size + calcifications suggest malignancy!
CT:
√ tumor attenuation typically > 10 HU
√ central areas of low attenuation ← tumor necrosis
√ heterogeneous enhancement (= foci of hemorrhage + central necrosis) + thin peripheral rim of enhancement
CECT:
√ peripheral nodular enhancement (in 88%)
√ venous tumor thrombus
√ relative percentage washout (RPW) of < 40% at 15 min
√ slow absolute washout of < 60% at 15 min
US:
√ well-defined round / oblong mass with lobulated contours
√ homogeneous echotexture in small tumor
√ complex echo pattern in large tumor with hyperechoic + hypoechoic regions ← hemorrhage + necrosis
MR:
√ tumor of low T1 signal + heterogeneously high T2 signal
√ heterogeneous areas hyperintense to liver on T1WI + T2WI ← internal hemorrhage + necrosis frequent:
√ high SI on T1WI ← methemoglobin
√ high SI on T2WI ← necrosis
√ loss of SI on out-of-phase imaging ← intracytoplasmic lipid
CEMR:
√ heterogeneous enhancement pattern with slow washout
√ nodular enhancement + central hypoperfusion
Angio:
√ neovascularity, occasionally with parasitization
√ AV shunting; multiple draining veins
NUC:
√ usually bilateral nonvisualization with 131I NP-59 (= carcinomatous side does not visualize because amount of uptake is small for size of lesion; contralateral side does not visualize because carcinoma is releasing sufficient hormone to cause pituitary feedback shutdown of contralateral gland)
PET:
√ hypermetabolic tumor on 18F-FDG with adrenal-to-liver max SUV ratio of > 1.45 (100% sensitive, 88% specific)
Biopsy: may appear histologically benign in well-differentiated adenocarcinoma
◊ Sampling error with fine-needle aspiration possible; use core biopsy instead
Prognosis: 0% 5-year survival rate
DDx: metastasis (similar signal intensities on MR); adrenocortical adenoma (mass of < 10 HU, >40% relative washout, > 60% absolute washout); myelolipoma (intralesional bulk fat)
Adrenocortical Neoplasm in Children
Incidence: 3÷1,000,000 annually; less common than neuro- blastoma but more common than pheochromocytoma
Mean age: 8 years (range, 6 months to 19 years); ²/³ younger than 5 years of age; M÷F = 2.2÷1.0
Path: adenoma = solitary spherical well-demarcated unencapsulated tumor of < 50 g
carcinoma = multinodular tumor with areas of hemorrhage + necrosis of > 100–500 g
Histo: NO reliable features to distinguish between adenoma and carcinoma!
Associated with:
(1) Beckwith-Wiedemann syndrome (3%)
2nd most common abdominal tumor after Wilms tumor
(2) Li-Fraumeni syndrome = SBLA (sarcoma, breast and brain tumors, laryngeal carcinoma, adrenocortical carcinoma)
• alteration of p53 tumor suppressor gene located on short arm of chromosome 17, band 13
(3) Familial Carney complex = cardiac myxoma + Sertoli cell tumor + adrenocortical neoplasm
(4) MEN 1 = pituitary prolactinoma + pancreatic islet cell tumor + parathyroid hyperplasia + adrenocortical neoplasm
• palpable abdominal mass (57%)
• gonadotropin-independent production of endogenous androgens + cortisol (92%):
• virilization in female
= herculean habitus (increased muscle mass), clitoromegaly, facial hair, advanced pubic + axillary hair development, advanced bone age
• isosexual precocious puberty in male
= early development of acne, pubic hair, penile enlargement
• mixed endocrine syndrome with cushingoid features (less frequent)
• other endocrine abnormalities (unusual):
• pure Cushing syndrome
• feminization in boys ← secretion of estrogen
• Conn syndrome (primary hyperaldosteronism)
• increase in 24-hour urinary ketosteroid excretion
• increased levels of serum cortisol, testosterone, androstenedione, estradiol
Metastases: lung > liver > tumor invasion of IVC (35%) > peritoneum (29%) > pleura + diaphragm (24%) > abdominal lymph nodes (24%) > kidney (18%)
US:
√ 3–22-cm round / ovoid well-circumscribed mass
√ lobulated border (common)
√ thin echogenic capsule-like rim (27%)
√ homogeneous mass hypo- / isoechoic to kidney
√ heterogeneous mass with centrally hypoechoic regions (= tumor necrosis) if large
√ tumor calcification (19%)
CECT:
√ well-circumscribed mass with thin rim
√ heterogeneous predominantly peripheral enhancement if lesion large
√ fine / coarse calcification (24%)
MR:
√ iso- / slightly hypointense to liver on T1WI
√ hyperintense to liver on T2WI
√ uniform signal loss at chemical shift imaging ← intracytoplasmic lipid
PET/CT:
√ hypermetabolic primary tumor + metastases
√ secondary findings ← excess serum cortisol of Cushing syndrome:
√ hyperattenuating / hyperechoic renal pyramids ← hypercalcemia
√ increase in retroperitoneal fatty tissue ← obesity
Rx: surgery
Prognosis of adrenocortical carcinoma:
survival rate of 70% [13%] for children < 5 years [> 5 years] of age; death within 1–2 years after diagnosis
| DDx: | (1) Neuroblastoma (encasing vascular structures, punctate calcifications, crosses midline, extradural extension through neural foramina, ill child, often already metastatic, increase in catecholamines) |
(2) Pheochromocytoma (older child, headaches) | |
(3) Adrenal hemorrhage (neonate, temporal evolution) | |
(4) Metastasis (extremely rare) |
ADRENOCORTICAL HYPERPLASIA
= ADRENAL CORTICAL HYPERPLASIA
◊ Responsible for 8% of Cushing syndrome and 10–20% of hyperaldosteronism!
Cause:
1. Corticotropin-dependent (85%): pituitary causes, ectopic ACTH production, CRF (corticotropin-releasing factor)production
2. Primary pigmented nodular adrenocortical hyperplasia
3. Primary aldosteronism (rare)
Prevalence: 0.51% increasing with age (autopsy); 4 x increased in patients with malignancy
Age: 70–80% in adults; 19% in children
Location: typically bilateral
Types:
(1) Smooth diffuse hyperplasia (common)
√ smooth to slightly lobular thickening of entire adrenal gland while maintaining its overall normal inverted-V or inverted-Y appearance
◊ In 45% of patients with Cushing syndrome
(2) Cortical nodular hyperplasia (less common)
Prevalence: increasing with age (autopsy)
Histo: mild nodularity (50%), distinct nodularity (15%)
Age: 65 years
Site: multifocal
√ focal hypo- to isoattenuating micro- / macronodules (= nodules up to 2.5 cm)
√ background of normal adrenal tissue / atrophic intervening cortex
◊ In 3% of patients with Cushing syndrome
Angio:
√ minimally increased hypervascularity
√ focal accumulation of contrast medium
√ normal venogram / may show enlarged gland
√ adrenal venous sampling to direct therapy in symptomatic patients ← results NOT ALWAYS CONCORDANT with imaging findings
NUC:
√ asymmetric bilateral NP-59 uptake (related to urinary cortisol excretion) WITHOUT dexamethasone suppression in Cushing syndrome
√ bilateral foci of NP-59 uptake WITH dexamethasone suppression (nondiagnostic ≥ 5 days)
Rx: no treatment in the absence of clinical / biochemical evidence of adrenocortical hyperfunction
ACTH-independent Macronodular Hyperplasia
= MACRONODULAR HYPERPLASIA WITH MARKED ADRENAL ENLARGEMENT
Etiology: unknown
• clinical features of hyperaldosteronism / Cushing syndrome
• suppressed ACTH ← active production of hormones
√ bilateral enlarged adrenal glands (often > 5 cm) with macronodules
Primary Pigmented Nodular Adrenocortical Disease
√ normal to slightly enlarged adrenals + small nodules + atrophy of intervening cortex
Associated with: Carney complex
ADRENAL REST TUMOR
= ADRENOCORTICAL REST
Prevalence: 7–15% of newborns; 1.6% of adults
◊ Adrenal rests only form masses after exposure to elevated levels of adrenocorticotropic hormone
Associated with conditions of ⇑ circulating ACTH:
(1) Congenital adrenal hyperplasia
(2) Cushing syndrome
(3) Addison disease
• increase in cortisol levels (testicular vein sampling is DIAGNOSTIC)
Location: near testicular hilum; usually bilateral
US:
√ multiple hypoechoic nodules
√ may become hyperechoic with acoustic shadowing
MR:
√ nodules isointense relative to normal testis on T1WI
√ nodules hypointense relative to normal testis on T2WI
√ diffuse enhancement after contrast administration
ADRENOGENITAL SYNDROMES
A. CONGENITAL TYPE = Congenital Adrenal Hyperplasia
= autosomal recessive enzyme defect
Incidence: 1÷15,000 in most white populations
Cause: mutation of CYP21A2 (in 90%)
Pathophysiology (in 90–95%):
21-hydroxylase deficiency → impaired cortisol + aldosterone synthesis → hyponatremia + hypokalemia + hypotension → ⇑ ACTH stimulation by pituitary gland (negative feedback mechanism) → ⇑ production of steroid precursors → diverted to production of androgens
Age: manifestation most often in neonatal period; M < F
Path: cerebriform appearance of cortical hyperplasia (weight increase to 2–4 x of normal); multilobular bilateral masses near rete testis (adrenocortical rests)
• excess of androgenic steroids:
› F: virilization of female fetus:
• pseudohermaphroditism (= clitoral hypertrophy, ambiguous external genitalia, urogenital sinus)
› M: precocious puberty in male → rapid growth at 3–7 years of age
• salt wasting ← diminished aldosterone production (in 75%):
• life-threatening hypovolemic salt-wasting adrenal crisis (during first 2 weeks of life)
@ Adrenal glands
√ ± symmetrically enlarged + thickened adrenal glands:
√ adrenal limb > 4 mm thick
√ coiled / cerebriform appearance
√ central echogenic stripe replaced by diffusely stippled echoes
√ massive bilateral myelolipomas ← long-standing / poorly treated congenital adrenal hyperplasia
@ Gonads (55%)
(a) females
√ typically normal gonads in females
√ cystic ovaries mimicking polycystic ovaries (76%)
(b) males
√ bilateral multinodular adrenocortical rests in rete testis (= mediastinum testis) in postpubertal boys (in 25%):
√ growth of adrenocortical rests ← effect of ACTH
√ usually hypoechoic < 5 mm masses
√ occasionally heterogeneously hyperechoic adrenals ± acoustic shadowing
√ iso- / slightly hyperintense on T1WI + hypointense on T2WI compared to adjacent testicular parenchyma
Rx: cortisone ± mineralocorticoids
B. ACQUIRED TYPE
M < F
(a) adrenal hyperplasia / adenoma / carcinoma: occasionally bilateral myelolipomas
(b) ovarian / testicular tumor
(c) gonadotropin-producing tumor: pineal, hypothalamic tumor, choriocarcinoma
• virilization; Cushing syndrome
ALKALINE-ENCRUSTED CYSTITIS AND PYELITIS
= chronic severe urinary tract infection affecting urothelial lining
Cause: nosocomial infection with urease-producing bacterium, most commonly Corynebacterium → producing alkaline urine
Predisposed: immunocompromised patient (esp. renal transplant patient), after invasive urologic procedure
Path: mucosal inflammation + encrustation of urothelial lining with struvite + calcium phosphate
• fever, hematuria, dysuria, suprapubic pain
• ammonia-like smell of urine
NECT:
√ diffuse thin / coarse superficial linear urothelial calcifications
Site: collecting system, ureter, bladder; often bilateral
Dx: culture positive > 48 hr for urea-splitting micro-organism
Cx: septic shock, graft failure
Rx: antibiotics, oral acidification of urine
AMYLOIDOSIS
= accumulation of extracellular eosinophilic amyloid protein
• gross hematuria (60%), urethral bleeding
• dysuria, frequency, cystitis, acute renal failure
GU location: bladder (50%), ureter (25%), urethra (20%), renal pelvis (6%)
@ Urinary bladder (50%)
Cause: ? chronic cystitis
Histo: stromal + muscle deposits of amyloid
• painless gross hematuria ← mucosal ulceration
• irritative symptoms
Site: posterior + posterolateral wall of bladder (68%) > multiple areas (65%)
√ nonspecific filling defects + distortion of bladder outline
√ CHARACTERISTIC linear submucosal / intramural calcifications
DDx: schistosomiasis mansoni, TB, urothelial carcinoma, other neoplasm
√ variable degrees of decreased contrast enhancement
√ decreased SI in bladder wall on T2WI
DDx: desmoplastic metastasis + bladder wall lymphoma (↓ T2-SI); urothelial carcinoma (↑ T2-SI)
@ Renal involvement
Frequency: 1° amyloidosis (35%),
2° amyloidosis (in > 80%)
• nephrotic-range proteinuria, renal insufficiency
√ smooth normal to large kidneys with increase in parenchymal thickness (acute stage)
√ small kidneys = cortical atrophy (in 50% of late stage)
√ occasionally attenuated collecting system
√ nephrographic density normal to diminished
√ amorphous renal calcifications
√ focal renal parenchymal mass lesions
US:
√ diffusely increased cortical echogenicity ← deposition of amyloid in glomeruli and interstitium
√ obscuration of arcuate arteries
√ preservation of corticomedullary differentiation
Cx: renal vein thrombosis → renal failure
@ Renal pelvis (6%)
√ calcification in submucosal deposit
√ irregular filling defect on excretory urography
√ hypointense amyloid deposit on T2WI (DDx: lymphoma, desmoplastic metastasis)
√ variable to NO enhancement
@ Ureter (25%)
Site: distal ureter; rarely bilateral
√ focal / diffuse areas of wall thickening + filling defects
√ irregular ureteral narrowing + stricture → hydronephrosis
√ linear submucosal / intramural calcifications
@ Urethra (rare)
• hematuria, dysuria, urethral obstruction
√ narrowing of urethra with filling defects
√ foci of increased echogenicity + posterior shadowing within corpus spongiosum
√ hypointense urethral + periurethral lesions on T2WI
Dx: urethroscopy + transurethral biopsy
DDx: urethral neoplasm
@ Seminal vesicles
= senile localized amyloidosis of seminal vesicles
Frequency: in 21% of men > 75 years of age (autopsy)
Site: symmetric involvement of both SV
DDx: invasion of SV by prostate cancer
Dx: transrectal biopsy
@ Retroperitoneum
√ diffuse infiltration encasing kidneys, aorta, IVC, pancreas
√ replacement of retroperitoneal fat with soft-tissue
√ focal retroperitoneal mass
MR:
√ intermediate T1 signal intensity
√ decreased T2 signal intensity
ANALGESIC NEPHROPATHY
= renal damage from ingestion of salicylates in combination with phenacetin / acetaminophen in a cumulative dose of 1 kg
Prevalence: USA (2–10%), Australia (20%)
Age: middle-aged; M÷F = 1÷4
• gross hematuria, hypertension
• renal colic (passage of renal tissue)
• renal insufficiency (2–10% of all end-stage renal failures)
• Analgesic syndrome: history of psychiatric therapy, abuse of alcohol + laxatives, headaches, pain in cervical + lumbar spine, peptic ulcer, anemia, splenomegaly, arteriosclerosis, premature aging
√ papillary necrosis
√ scarring of renal parenchyma (“wavy outline”); bilateral in 66%, unilateral in 5%
√ renal atrophy
√ papillary urothelial tumors in calices / pelvis (mostly TCC / squamous cell carcinoma), in 5% bilateral
ANGIOMYOLIPOMA
= AML = Renal choristoma (= benign tumor composed of tissues not normally occurring within the organ of origin)
N.B.: normal cells / tissues in an abnormal location!
[= Renal Hamartoma (improper name since fat and smooth muscle do normally occur within renal parenchyma]
= most common benign mesenchymal tumor of kidney composed of varying admixtures of thick-walled blood vessels, smooth muscle cells and mature fat (→ hence name!)
Prevalence: 0.3–2.0% of all renal tumors; 1% of all surgically removed renal tumors
| Genetics: | (a) sporadic (50–70%) |
(b) inherited with tuberous sclerosis (30–50%), neurofibromatosis, vHL syndrome |
Path: large infiltrating necrotic tumor without true capsule, 88% extending through renal capsule, hemorrhage (characteristic lack of complete elastic layer of vessels predisposes to aneurysm formation); tumor continues to grow during childhood + early adulthood
Histo:
(a) classic triphasic (92%): tumor composed of mature fat, aggregates of dysmorphic / thick-walled blood vessels, epitheloid immature smooth muscle; coexpresses melanocytic markers (HMB-45, melan-A) and smooth muscle markers (smooth muscle actin, calponin), negative for epithelial markers
(b) monophasic epitheloid (8%): high degree of association with tuberous sclerosis + aggressive behavior
Average age: 41 years; M÷F = 1÷2
• small lesions are asymptomatic (60%)
• acute flank / abdominal pain in 87%
◊ Angiomyolipomas > 4 cm are symptomatic in 82–94% ← spontaneous bleeding in 50–60%!
• gross hematuria, anemia, hypertension
• Wunderlich syndrome = hemorrhagic shock ← massive bleeding into angiomyolipoma or into retroperitoneum (10%)
Location: renal parenchyma; renal hilum; may be exophytic perirenal / completely extrarenal (retroperitoneum, solid + hollow organs, skin, gynecologic region)
Mean size: 9 cm (range, few mm to 30 cm) in diameter
√ hypervascular mass with large feeding arteries, multiple aneurysms, laking without shunting, tortuous circumferential vessels, whorled parenchymal + venous phase
US:
√ homogeneously echogenic mass similar to sinus fat (DDx to renal cell carcinoma)
CT:
(a) ordinary AML (in 95%):
√ negative attenuation values
◊ Even a small amount of fat within a solid mass on NECT secures the diagnosis!
(b) minimal-fat AML (in 5%)
= angiomyolipoma with microscopic fat only mimicks RCC
√ hyperattenuating (53%) / isoattenuating (26%) / hypoattenuating (21%) mass (DDx: RCC)
√ homogeneous prolonged tumor enhancement
MR:
√ markedly hyperintense adipose tissue relative to renal parenchyma + isointense relative to fat on T1WI
√ demonstration of fat on selective fat-suppression sequence
√ prominent signal loss relative to other tissues on fat-suppressed / opposed-phase images with respect to in-phase images ← intravoxel coexistence of fat and water:
√ characteristic India ink artifact at interface between mass and normal renal parenchyma on opposed-phase T1WI
√ central portions of lesion do not demonstrate changes in signal intensity compared with in-phase images
√ variable SI on T2WI:
√ homogeneously high SI at single-shot T2WI with large fatty mass
√ homogeneously low SI relative to renal parenchyma in lipid-poor angiomyolipomas on T2WI
√ decreased signal intensity on Gd-enhanced images (DDx: RCC enhances)
| Cx: | (1) Hemorrhage with spontaneous rupture (25%) ← tumor > 4 cm / intratumoral aneurysm > 5 mm |
(2) Growth into renal vein / IVC |
◊ Not necessarily implying malignant transformation
(3) Renal failure
| Rx: | (1) Annual follow-up of lesions < 4 cm |
(2) Semiannual follow-up of lesions ≥ 4 cm | |
(3) Emergency laparotomy (in 25%): nephrectomy, tumor resection | |
(4) Selective arterial embolization with hemorrhage | |
(5) Prophylactic surgery in pregnant women | |
(6) Screening for tuberous sclerosis |
DDx: renal / perirenal lipoma or liposarcoma; Wilms tumor / renal cell carcinoma (occasionally contains fat if large, but also calcium); clear cell RCC with small amount of intracellular fat
Isolated Angiomyolipoma (50–70%)
= SPORADIC ANGIOMYOLIPOMA
Mean age: 43 (range, 27–72) years; M÷F = 1÷4
• flank pain, hematuria, palpable mass
√ solitary + unilateral (in 80% on R side) AML, NO stigmata of tuberous sclerosis
√ stable over long periods of time
Angiomyolipoma Associated with TS (30–50%)
Mean age: 17 years; usually present by 10 years; M÷F = 1÷1
◊ In 70–80–95% of patients with tuberous sclerosis
◊ May be the only evidence of tuberous sclerosis
√ commonly large + bilateral + multifocal AMLs with macroscopic fat
√ tendency for growth + hemorrhage
ARTERIOVENOUS RENAL CONNECTION
√ early enhancement of draining vein + renal vein + IVC
√ intraparenchymal / subcapsular / perirenal hematoma (as a result of bleeding)
Rx: transcatheter intraarterial occlusion, surgery
Arteriovenous Malformation (20–30%)
| Cause: | (1) Congenital AVM |
(2) Acquired AVM: trauma, spontaneous rupture of aneurysm, very vascular malignant neoplasm |
Histo:
(a) cirsoid AVM = multiple coiled vascular channels grouped in cluster
(b) cavernous AVM = single well-defined artery feeding into a single vein (rare)
• gross hematuria
Location: adjacent to collecting system
√ large unifocal mass:
√ focally attenuated and displaced collecting system
√ homogeneously enhancing mass
√ curvilinear calcification
√ supplied by multiple segmental / interlobar arteries of normal caliber
√ draining into one / more veins
US:
√ tubular anechoic structure (DDx: hydronephrosis, hydrocalyx)
Cx: subcapsular / perinephric hematoma (rare)
Arteriovenous Fistula (70–80%)
M > F
| Cause: | (1) Acquired: trauma (stab wound, percutaneous needle biopsy, percutaneous nephrostomy, nephrolithotripsy), surgery, tumor, inflammation, erosion of aneurysm into vein |
(2) Idiopathic |
Path: single dilated feeding artery + single draining vein
• asymptomatic with abdominal bruit / abdominal pain
• persistent / delayed gross hematuria (common)
√ tortuous varices over time
√ enlargement of renal vein
US:
√ focal area of aliasing / color saturation ← high flow rate + vessel tortuosity
√ ⇑ flow velocity + ⇓ resistance in feeding artery
√ arterial pulsations in draining vein
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


