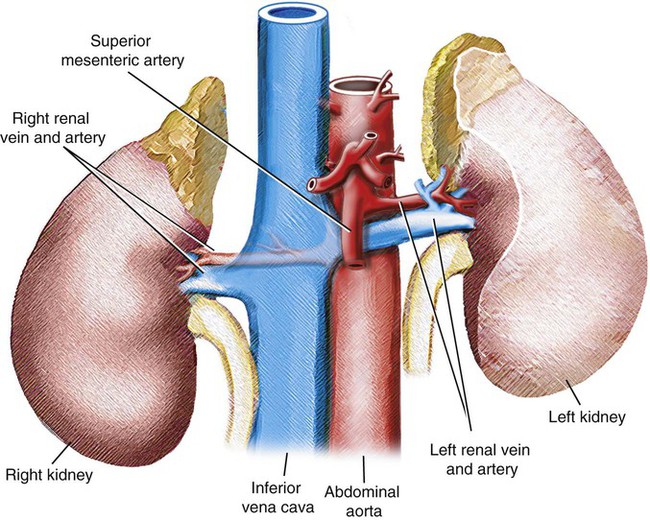
The adrenal glands lie at the anterosuperior aspect of the upper pole of each kidney and are enclosed within the renal fascia but separated from the kidneys by loose fibroareolar tissue (Fig. 109-1). There maybe several small masses of tissue identical with adrenal cortex “cortical bodies” in the neighborhood of the gland. The right adrenal gland is roughly triangular, with its apex and medial portion of the anterior surface in contact with the posterior aspect of the inferior vena cava (IVC) (Fig. 109-2
Adrenal Venous Sampling
Technique
Anatomy and Approach
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine






