Fig. 16.1
Representative 3D images of the right ventricle of a patient with arrhythmogenic right ventricular cardiomyopathy (ARVC). Orthogonal long-axis views of the right ventricle (top), short-axis view (bottom left), 3D view (bottom right) (Modified from Prakasa et al. [4], with permission)
16.3 Tissue Doppler Imaging
Tissue Doppler imaging (TDI), if applied to RV walls, allows quantitative assessment of RV longitudinal function by measuring myocardial velocities and velocity-derived deformation parameters (strain and strain rate). Owing to its theoretical ability to assess regional contractile function, TDI can provide important information in ARVC, considering the dyshomogeneous nature of myocardial involvement in this peculiar type of cardiomyopathy. Furthermore, this technique demonstrates the potential of detecting subtle impairment in a given myocardial segment, which are missed by standard echocardiographic parameters [7–9].
A simple and quick application of pulsed TDI is the measurement of tricuspid annular velocity, which reflects RV longitudinal contraction. Interestingly, in one study on ARVC patients, tricuspid annular systolic tissue velocity was the echocardiographic parameter that correlated best with RV EF assessed by CMR [10].
Regional myocardial velocities can be measured simultaneously in the three segments of the RV free wall (base, mid, and apex) using color-coded TDI images, which are usually recorded in the apical four-chamber view and subsequently processed offline. To obtain accurate myocardial velocities, sample regions of 3- to 5-mm in diameter should be placed in the basal part of the segment and on the endomyocardial side in end-systole [11].
Other potentially important information is the assessment of RV strain and strain rate by TDI. These deformation parameters have correlated closely with invasive measures of contractility [12], and reference values for both RV TDI velocities and strain are reported in normal individuals [13].
In a cohort of ARVC patients, Teske et al. [14] demonstrated that the lowest strain value in any of the three segments of the RV free wall had the best diagnostic accuracy when using a cutoff value of −18.2 % (Fig. 16.2). This parameter was superior to all conventional echocardiographic measures for functional and structural RV alterations. Furthermore, this method seems to eliminate almost entirely the false-positive findings on visual assessment of regional function, primarily due to the presence of hypokinesis in the basal or mid segment of the RV free wall or dyskinesis in the apical region.
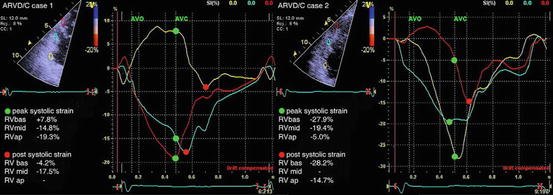
Fig. 16.2
Tissue-Doppler-imaging assessment of right ventricular (RV) strain in two cases of arrhythmogenic right ventricular cardiomyopathy (ARVC). In case 1 (left), RV basal segment (RVBAS) (yellow curve) is most affected (dyskinetic), with a normal function in the RV apical segment (RVAP) (red curve). In case 2 (right), normal peak systolic values are found in RVBAS (yellow curve) and RV mid segment (RVMID) (blue curve), but RV apical segment (RVAP) (red curve) shows an abnormal deformation pattern. AVC arterial (pulmonic) valve closure, AVO arterial (pulmonic) valve opening (Adapted from Teske et al. [14], with permission)
Nevertheless, although this technique seems to offer a more accurate assessment of regional function over standard 2D echocardiography and has been applied extensively for research purposes, its use in clinical practice is limited by a variety of factors. One of the most important is that TDI is an angle-dependent technique, and appropriate alignment with the vector of contraction is needed in order to obtain reliable measurements. Furthermore, acquisition is conditioned by a series of artifacts, and processing is time consuming.
16.4 Speckle-Tracking Echocardiography
Speckle-tracking echocardiography can be used for quantitative functional assesment of both LV and RV. As longitudinal RV shortening is a more important contributor to RV systolic function compared with circumferential shortening [15], most experience with RV speckle-tracking echocardiography is with regional and global longitudinal strain and strain-rate assessment (Fig. 16.3, Clips16.1).
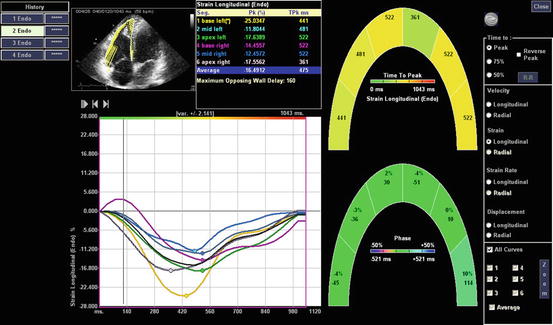
Fig. 16.3
Assessment of right ventricular (RV) longitudinal strain and strain rate by speckle-tracking echocardiography in a patient with arrhythmogenic right ventricular cardiomyopathy (ARVC) using a six-segment model from an apical four-chamber view. Regional longitudinal strain and strain-rate values are shown for each segment, and average values are automatically provided. Of note, global longitudinal strain results are significantly reduced (−16 %) in this patient
RV data acquisition for speckle-tracking analysis is performed with a 2D echocardiographic probe in the apical four-chamber view, and data are subsequently processed offline. Different software allow endocardial border tracing in a semiautomatic or manual mode, usually at end-systole. RV is automatically divided into six segments: base, mid, and apex of the RV free wall and septum, respectively, and segmental and global longitudinal strain and strain rate are calculated (Fig. 16.3, Clips 16.1).
Speckle-tracking echocardiography applied in ARVC shows significantly reduced RV global longitudinal strain in the affected population compared with normal controls [14
 Dilated Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
Dilated Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
 Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
 Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
 Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
 Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
 Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management
Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management




Related posts:
Dilated Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
