Fig. 11.1
Patient with hypertrophic cardiomyopathy: M-mode echocardiography (a) shows a severe left ventricular (LV) septal hypertrophy (24 mm) with preserved systolic function evaluated with conventional echocardiographic indices (fractional shortening 35 %, ejection fraction 63 %). Apical four-chamber view (b) demonstrates moderate biatrial dilatation; in the right chambers, the lead of the implantable cardioverter defibrillator (ICD) is visible. Doppler interrogation of the transmitral valve (c) shows a restrictive filling pattern (E wave = 80 cm/s, E wave deceleration time = 115 ms). Tissue Doppler imaging curve on the septal mitral valve annulus (d) shows low systolic wave velocities (S’ = 4 cm/s) and early diastolic wave (E’ = 4 cm/s). E/E’ = 20
Early diastolic mitral annular velocity (E’), a relatively pre-load-independent index of LV relaxation, is usually reduced in patients with HCM (Fig. 11.1) compared with age-matched controls and relates to LV hypertrophy magnitude [3]. As shown by Nagueh et al. [1], peak systolic myocardial velocity at TDI (S’) and early diastolic velocity (E’) are also reduced in patients with subclinical disease (early phenotype) in comparison with normal controls.
The use of TDI can also assist in differentiating between variants of LV hypertrophy. Vinereanu et al. [4] used TDI to distinguish pathological from physiological LV hypertrophy in a study comprising patients with HCM, patients with systemic hypertension, athletes, and normal individuals. Long-axis systolic and early-diastolic velocities were decreased in patients with pathologic hypertrophy but preserved in athletes. Heterogeneity of annular velocities discriminated between hypertensive patients and HCM.
Evaluation of the E to /E’ ratio (E/E’) using transmitral Doppler and TDI has allowed noninvasive estimation of LV filling pressures in various cardiac disease patient populations [5]. On the contrary, in symptomatic patients with HCM, Doppler echocardiographic estimates of LV filling pressure using E/E’ correlate only modestly with direct measurement of left atrial (LA) pressure [6]. Nevertheless, E/E’ has been correlated with exercise tolerance in adults (with an inverse correlation with peak oxygen consumption) [7] and children [8] with HCM. In addition, septal E’ velocity appears to be an independent predictor of death and ventricular arrhythmia in children with HCM [8].
TDI assessment of regional myocardial function has some important limitations because of its angle dependence (as with all Doppler techniques) and because it measures absolute tissue velocities and not myocardial deformation, being consequently influenced by cardiac translational motion and tethering. These limitations led to the development of more sophisticated echocardiographic techniques, such as TDI-derived myocardial strain and strain rate and speckle-tracking imaging.
11.2.1 Tissue-Doppler-Imaging-Derived Strain
Longitudinal myocardial strain and strain rate can be estimated by TDI technique and can provide useful information on local myocardial motion or deformation relative to the adjacent myocardium [9]. One of the first studies on strain in HCM was by Yang et al. [10], who reported the assessment of regional myocardial function in 31 adults with HCM diagnosed echocardiographically. Longitudinal strain was evaluated at the basal, mid, and apical segments of septal and lateral walls. It was significantly reduced in the septal segments of patients with HCM compared with control patients. More importantly, within the septum, midseptum longitudinal strain was significantly diminished compared with basal and apical segments. Kato et al. [11] demonstrated a major role of strain rate in differentiating nonobstructive HCM from hypertensive LV hypertrophy. The authors compared an HCM population and hypertensive patients and showed that at multivariate analysis, systolic strain rate and interventricular septum (IVS)/posterior wall thickness ratio were the most powerful predictors for the diagnosis of HCM. However, TDI-derived strain imaging also has technical limitations due to its angle dependence and frequent artifacts.
11.2.2 Speckle-Tracking Imaging
Speckle-tracking echocardiography, relatively a new imaging technique that allows objective and quantitative evaluation of global and regional myocardial deformation independently from the angle of insonation and from cardiac translational movements [12], has been employed in HCM in various settings. Serri et al. [13] applied 2D strain echocardiography to a subset of patients with familial nonobstructive HCM. Despite apparently normal systolic function (with the use of standard criteria), all components of strain (longitudinal, transverse, circumferential, radial) were significantly reduced in HCM in comparison with a healthy control population. Carasso et al. [14] showed that patients compared with controls had higher circumferential strain and lower longitudinal strain. In addition, mid-LV rotation was clockwise (opposite to normal). LV outflow-tract (OT) obstruction and clinical status were related to more circumferentially directed strain and reduced apical biplanar strain.
The ability of predicting the presence of myocardial fibrosis in HCM patients using echocardiography could have important implications, especially when predicting adverse outcomes, such as sudden death (SD). Funabashi et al. [15] used speckle-tracking echocardiography and cardiac magnetic resonance (CMR) to study 29 HCM patients. The authors showed that absolute peak longitudinal strain values were significantly lower in fibrotic lesions than in nonfibrotic lesions (Fig. 11.2). Moreover, there is an inverse association between various histopathologic findings typical of HCM (myocyte hypertrophy, disarray, small intramural coronary arteriole dysplasia, interstitial fibrosis) and septal strain rate in symptomatic HCM patients who undergo surgical myectomy, as demonstrated by Kobayashi et al. [16]. It is thus possible that myocyte disarray is related to a abnormal ventricular architecture that predisposes to worsening regional LV function. Saito et al. [17] showed that global longitudinal strain might provide useful information regarding myocardial fibrosis [correlating with late gadolinium enhancement (LGE) at CMR] and cardiac events in HCM patients with normal systolic function. Strain imaging of the LA allows for a more direct assessment of LA function. LA longitudinal function, quantified using TDI and 2D strain in HCM patients, was reduced compared with non-HCM patients with LV hypertrophy due to other conditions, as well as with healthy controls [18].
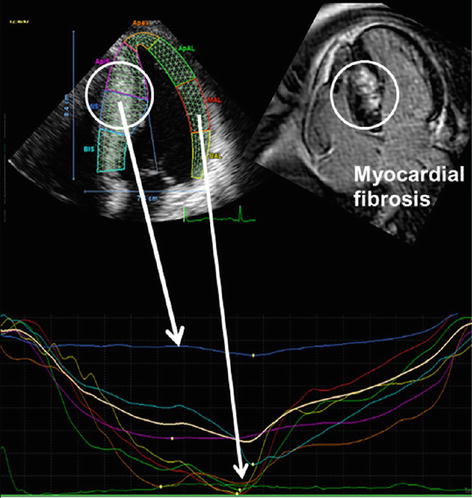
Fig. 11.2
Longitudinal strain measurement in seven left ventricular segments from an apical four-chamber view (upper left), regional strain curves (bottom), and cardiac magnetic resonance (CMR) (upper right) in hypertrophic cardiomyopathy patient with fibrosis in the interventricular septum. The segments with fibrosis at CMR show lower longitudinal strain values (less negative) compared with segments without fibrosis (From [15], with permission)
The role of 3D speckle-tracking echocardiography has also been evaluated in HCM. In particular, in the study by Baccouche et al. [19] comparing cardiac amyloidosis (CA) and HCM, basal radial strain was significantly reduced in the former condition (Fig. 11.3). Moreover, in HCM, 3D speckle-tracking parameters showed a remarkably weaker correlation with LGE compared with individuals with CA. This is most likely explained by the focal character of fibrosis, which may be less accessible for 3D strain imaging compared with amyloid changes.
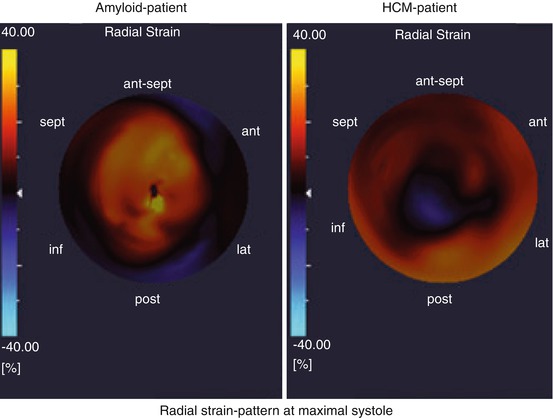
Fig. 11.3
Sixteen-segment polar maps (bull’s-eye plot) of 3D speckle-tracking radial strain in a patient with cardiac amyloidosis (left) compared with a patient with hypertrophic cardiomyopathy (right). The basoapical radial strain gradient displays opposite characteristics in the two diseases: in cardiac amyloidosis, basal radial strain is significantly reduced, with a gradual increase from base to apex; hypertrophic cardiomyopathy shows a physiological gradient of basoapically decreasing radial strain. ant anterior, ant-sept anteroseptal, HCM hypertrophic cardiomyopathy, inf inferior, lat lateral, post posterior, sept septal (From [19], with permission)
11.3 Three-Dimensional Echocardiography
Another significant advancement in the field of echocardiography is the development and refinement of 3D echocardiography, which can provide insights into mechanics of LV obstruction, LV architecture, and mitral and aortic structure and function. One major advantage of 3D echocardiography is the improved accuracy in evaluating cardiac chamber volumes by eliminating the need for geometric modeling and the errors caused by foreshortened apical views [20].
One of the most common features of HCM is LV obstruction, which is often complex in nature, involving MV leaflets, papillary muscles, and the hypertrophied septum [21]. As demonstrated by Song et al. [22
 Dilated Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
Dilated Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
 Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
 Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
 Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
 Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
 Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management
Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management




Related posts:
Dilated Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
