actual practice in the moving, crying infant. To help solve this problem, a variety of immobilization devices are available for children <4 years old. Pacifiers are also useful. An important caveat is that pediatric patients with suspected airway obstruction should never be forced into a position they do not wish to assume, because this may lead to acute respiratory decompensation, which is potentially life threatening.
 FIGURE 8.1 Position for lateral airway radiography in an infant. The lateral radiograph is obtained in deep inspiration with the neck extended. Radiographer can stabilize the optimal neck position of the patient while obtaining the neck radiograph. |
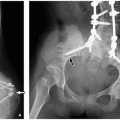
 FIGURE 8.2 Lateral and anteroposterior airway radiographs. A: Lateral radiograph shows normal degree of oropharyngeal distension, “small finger-sized” epiglottis (curved arrow) and thin aryepiglottic folds (straight arrow). Moderate enlargement of adenoids (asterisk) is also seen. B: Anteroposterior airway radiograph demonstrates normal symmetric subglottic “shoulders” (arrows). |
 FIGURE 8.3 Well-coned anteroposterior chest radiograph. Radiographer can stabilize the child for the optimal chest position while obtaining chest radiograph. Note the lead drape over the lower abdomen. |
 FIGURE 8.4 Suboptimal quality lateral airway radiograph due to overlying earrings and fingers with suboptimal neck extension obtained in expiration. Widening (asterisk) of the retropharyngeal soft tissues during expiration may mimic a retropharyngeal abscess. |
TABLE 8.1 Radiography Technique for Soft Tissue Neck | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 FIGURE 8.5 Positioning for upright chest radiograph in cooperative older children. Posteroanterior (A) and lateral (B) radiograph in an upright position can be obtained in sitting position and with the arm elevated. |
 FIGURE 8.6 Normal chest radiograph in an older child. A: Posteroanterior chest radiograph shows trachea (T), carina (C), and bilateral mainstem bronchi (B). B: Lateral chest radiograph demonstrates trachea (T) and carina (C). |
 FIGURE 8.7 Chest radiographs obtained at end inspiration and end expiration in a 5-year-old girl. This patient was subsequently diagnosed a nonradiopaque foreign body lodged in the left mainstem bronchus by bronchoscopy. A: Frontal chest radiograph obtained at end inspiration shows fairly symmetric lung aeration. B: Frontal chest radiograph obtained at end expiration demonstrates expected decreased right lung volume but substantial hyperinflation of the left lung indicating underling air trapping due to left mainstem bronchial obstruction. |
 FIGURE 8.8 Value of lateral decubitus view. A 2-year-old girl who presented with acute wheezing and coughing after playing with her brother’s plastic building toys. The patient was subsequently diagnosed with a nonradiopaque foreign body lodged in the left mainstem bronchus by bronchoscopy. A: Frontal radiograph shows mildly hyperinflated left lung compared to the right lung. B: Left-sided lateral decubitus view demonstrates persistent hyperinflation of the left lung. |
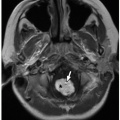
 FIGURE 8.9 Normal trachea seen on ultrasound. Air within the nondependent portion of the trachea (T) in supine position of the patient shows increased echogenicity (arrow) with posterior shadowing. Also seen is normal thyroid gland (asterisks) on both sides of the trachea. |
(representative parameters: 5,000/34, echo train length of 12, 22-cm field of view, 6-mm section thickness with 2-mm gap, 256 × 192 matrix, two signals acquired) sequences are obtained. Cine MR is performed in midline sagittal and axial planes at the midportion of the tongue using a fast gradient-echo sequence (representative parameters: 8,200/3,600, 80-degree flip angle, 12-mm section thickness) with 128 consecutive images captured in ˜2 minutes and viewed on cine mode.2,16
 FIGURE 8.10 Tracheomalacia in a 4-year-old girl who presented with chronic cough and recurrent pulmonary infection. Subsequently performed bronchoscopy confirmed the diagnosis of marked tracheomalacia. A: Lateral radiograph obtained at end inspiration during airway fluoroscopy study of airway shows patent trachea (arrows). B: Lateral radiograph obtained at end expiration during airway fluoroscopy study demonstrates marked (>75%) collapse of the trachea (arrows), consistent with tracheomalacia. |
and soft palate, uvula, oropharynx, tongue, mandible, base of the tongue, vallecula, epiglottis, aryepiglottic folds, pyriform sinuses, laryngeal ventricle, true and false vocal cords, subglottic larynx, and upper trachea (Fig. 8.2).
 FIGURE 8.11 Normal large airway in a 6-year-old girl. A: Enhanced axial CT image at the aortic arch level shows normal round and patent trachea (T) obtained at end inspiration. (A, aortic arch; SVC, superior vena cava; E, esophagus.) B: Enhanced axial CT image shows normal and patent bilateral mainstem bronchi (MB). (AA, ascending aorta; DA, descending aorta; SVC, superior vena cava; LP, left main pulmonary artery.) C: Sagittal reformatted lung window CT image of the large airway. A reference line (yellow line and red asterisks) through the center of the airway for reconstruction of a curved coronal reformatted CT image. D: Curved coronal reformatted CT image shows a straightened view of the entire trachea. E: 3D external volume-rendered CT image (i.e., virtual bronchography) of normal airway. (Continued) |
 FIGURE 8.11 (Continued) F: 3D internal volume-rendered CT image (i.e., virtual bronchoscopy) of airway obtained at glottis level. Mildly opened glottis is seen. G: 3D internal volume-rendered CT image of airway obtained at the level of carina. Bilateral mainstem bronchi are patent. |
TABLE 8.2 Tube Current and kV by Patient Weight for Central Airway MDCT | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
breathers.2 Associated anomalies such as coloboma, heart defects, and mental retardation and syndromes including CHARGE (coloboma, heart disease, choanal atresia, growth and mental retardation, genital hypoplasia, ear anomalies with deafness), Crouzon, Pfeiffer, Antley-Bixler, Marshall-Smith, Schinzel-Giedion, and Treacher Collins occur in ˜50% of affected patients.2,21,23
 FIGURE 8.12 Normal anatomy of the upper airway. T1-weighted sagittal MR image shows normal anatomy of the upper airway. |
 FIGURE 8.13 Normal bronchial anatomy. |
nasopharyngeal and oropharyngeal obstruction. Potential sequelae include chronic hypoxemia and hypercarbia from hypoventilation and OSA.2,14,33,34,35,36,37
 FIGURE 8.14 Normal lobar anatomy. |
 FIGURE 8.15 Normal trachea deviation (also known as buckling) in an 11-month-old boy who underwent chest radiograph for fever and cough. Coned radiograph shows normal deviation (arrow) of the trachea to the right of midline at the thoracic inlet level. |
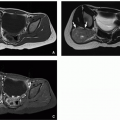
 FIGURE 8.16 Osseous type choanal atresia in a newborn boy who presented with respiratory distress and inability to pass a nasogastric tube. Axial bone window CT image of the facial bones shows bony obliteration of both choanae with diamond-shaped vomers (arrows). Accumulated secretions (asterisks) are also present in the dependent potions of the nasal passages. |
 FIGURE 8.17 Membranous type of choanal atresia. Axial bone window CT image of the facial bones in a newborn girl who presented with respiratory distress shows narrowed posterior choanae on the right side with soft tissue density (arrow) compatible with right-sided membranous type of choanal atresia. Left-sided posterior choanae (asterisk) is normal and patent. |
enlargement, particularly when associated with airway compromise or OSA, adenoidectomy and/or tonsillectomy may be required. Surgery may also help relieve associated recurrent sinus or ear infections.2
 FIGURE 8.18 Congenital pyriform aperture stenosis in a newborn girl who presented with dyspnea while feeding. Axial bone window CT image of the facial bone shows marked narrowing (circled area) of the nasal passages anteriorly due to closed apposition of the maxilla anteriorly. |
 FIGURE 8.19 Adenoid, palatine, and lingual tonsillar hypertrophy in a 12-year-old girl who presented with progressively worsening oral breathing and snoring. Lateral radiograph of the upper airway shows moderate prominence of the adenoids (asterisk) causing narrowing of the nasopharynx. There is also substantial enlargement of the lingual tonsils (arrowhead) and palatine tonsils (arrow). |
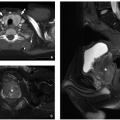
 FIGURE 8.20 Macroglossia in a 4-year-old boy with Down syndrome and respiratory distress. A sagittal T2-weighted MR image shows a large tongue (asterisk) without abnormal internal signal. Glossoptosis or posterior displacement of the tongue is also seen (arrows). |
 FIGURE 8.21 Laryngomalacia in a 2-month-old infant with stridor. A: Lateral radiograph of the upper airway demonstrates the normal position of the epiglottis (arrow). B: Lateral radiograph of the upper airway shows laxity of the epiglottis (arrow) with posterior and downward movement obstructing the airway. (Reprinted from Laya BF, Lee EY. Congenital causes of upper airway obstruction in pediatric patients: updated imaging techniques and review of imaging findings. Sem Roentgenol. 2012;47(2):147-158, with permission. Case courtesy of Khristine Grace C. Pulido, MD, Manila, Philippines.) |
trapping, persistent cough, stridor, acute respiratory distress, or hemoptysis.63,64 A classic history is persistent right upper lobe atelectasis following endotracheal intubation because of obstruction of the unsuspected aberrant bronchus by the endotracheal tube.25,26
 FIGURE 8.22 Diagram of three types of congenital tracheal agenesis. In congenital tracheal agenesis type I, the proximal trachea is atretic. The preserved short distal trachea communicates with the esophagus via a tracheoesophageal fistula. In congenital tracheal agenesis type II, the trachea is nearly or entirely absent. Two main bronchi join to form a midline carina, which most often fistulizes with the esophagus. In congenital tracheal agenesis type III, the trachea and carina are absent. The main bronchi arise directly from the distal esophagus at separate origins. |
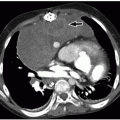
 FIGURE 8.23 Tracheal agenesis in a 3-day-old boy with multiple congenital malformations including DiGeorge syndrome, tetralogy of Fallot, right aortic arch, and discontinuous pulmonary artery who presented with severe respiratory distress. A: Frontal chest radiograph shows a missing tracheal air column. B: Enhanced axial CT image shows an absent trachea and right mainstem bronchus (arrow) directly arising from the distended esophagus (E). Also noted is a nasogastric tube within the esophagus. (Case courtesy of Jonathan R. Dillman, MD, MSc, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH.) |
 FIGURE 8.24 Tracheal bronchus in an 11-month-old boy who presented with a history of recurrent right upper lobe atelectasis and infection. Subsequently obtained bronchoscopy confirmed an abnormal bronchus arising from the right lateral wall of the trachea. A: Enhanced axial soft tissue window CT image shows an anomalous right upper lobe bronchus (arrow), tracheal bronchus, arises directly from the lateral wall of the trachea (T). B: 3D external volume-rendered CT image of the large airways and lungs confirms the origin and course of the tracheal bronchus (arrow). C: 3D internal volume-rendered CT image shows an opening (arrow) of the tracheal bronchus located above the carina. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


