Location: Deep-seated, lower limb within the muscle, thigh.
Clinical: Globose or multinodular mass, slowly increasing, and painless. Tumor may be large, present from many years, and richly vascularized with pulsation on the mass.
Imaging: On CT: an intense uptake of contrast medium. On angiography: tumoral neoangiogenesis and indirect signs of arteriovenous shunt. On MRI: bright on both T1 and T2, homogeneous on the first and inhomogeneous with sharp peripheral demarcation of the mass on the second.
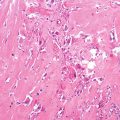
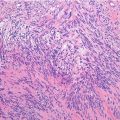
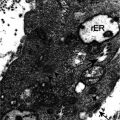
Histopathology: Soft, yellowish-white, or gray-red-purple, with hemorrhagic and necrotic areas, poorly delimited. Typical very glandular, acinar, and alveolar appearance. Nests of tumor cells are separated by thin-walled vascular spaces. Cells are large, epithelioid, globose-polyhedric, with eosinophilic granular to clear cytoplasm. The nucleus is vesicular, the nucleolus evident, mitotic figures rare, pleomorphism and hyperchromia, and sporadic giant cells with monstrous nuclei. Intense neoangiogenesis and frequent vascular invasion. At genetic level, this tumor is characterized by an unbalanced translocation: der(17)t(X;17)(p11;p25), resulting in the fusion of a gene of unknown function ASPL on chromosome 17 to the TFE3 transcription factor gene on the X chromosome.
Course and Staging: Recurrences are frequent when treated inadequately. Metastases may be present at diagnosis and at the first signs of the lesion. At times, they occur very late, even 10 years after the diagnosis. Usually, stage II B or III B.
Treatment: Wide or radical excision associated to adjuvant radio- and/or chemotherapy.
Chromosomal Translocations
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


