CHAPTER 15 An introduction to diverticular disease




Introduction
The origin of the word diverticulum is suggested to come from the Latin de-verto – to turn aside, at that time implying a by-road (Google, 2008), although perhaps more memorably it has been suggested that it related to a ‘wayside house of ill repute’ (Tjandra et al., 2008). Nowadays, it is associated with a benign sac-like protuberance that arises from a hollow organ.
History
Diverticula of the colon were first described by Littre in 1700. The possibility of diverticula as a site of infection and perforation was first raised in 1849 by Jean Cruveilhier, an eminent Parisian anatomist (Painter and Burkitt, 1971; Mimura et al., 2002). In 1912, George Haenisch, a roentgenologist, was the first to recognize and describe diverticulitis radiologically.
When considering the etiology of diverticular disease, the most substantiated theory is that of a deficiency in dietary fiber. Following his work as a surgeon in central Africa in the 20th century, Dennis Burkitt appreciated the connection between dietary fiber and the volume and soft nature of feces produced with negligible discomfort by the Africans who lived largely on a vegetarian diet. In 1971, Painter and Burkitt put forward their belief that a low-residue diet was the cause of diverticular disease. It was also noted at that time that, in the central parts of Africa, a number of diseases common in the West, including diverticulitis, were rarely observed (Painter and Burkitt, 1971; Story and Kritchersky, 1994; Netter, 2000; Mimura et al., 2002; Stollman and Raskin, 2004).
Anatomy: colon structure as it relates to diverticular disease
To understand the mechanism of how and why diverticula can form, the musculature and blood supply of the colon need to be reviewed. The colon is made up of four layers: mucosa, submucosa, muscularis and serosa. The muscular layer consists of an inner circular muscle and external longitudinal muscle. The circular muscle forms a thin layer over the cecum and colon, forming a thicker layer covering the rectum. The external longitudinal muscle forms a coating of muscle fiber much thinner than that of the circular muscle it covers. On three aspects of the circumference of the colon, the muscle thickens to form three longitudinal bands, the teniae coli. Individually, the muscle bands are known as tenia mesocolica, libera and omentalis. The three teniae are shorter than the length of circular muscle causing the colon to concertina and become sacculated. These sacculations are called haustral folds between which circular muscle fiber becomes thicker. The three teniae have their origin of attachment at the base of the appendix. In most cases, the bands are spaced equidistant around the circumference of the cecum (Davies, 1969; Netter, 1975) (see also Chapter 4).
In the distal colon, the three teniae fan out at the level of the peritoneal reflection, completely encasing the rectum but forming a thickened portion still recognizable as bands on the anterior and posterior aspects of the rectum (Wolf et al., 2000). Diverticula do not occur distal to the peritoneal reflection, as the anatomical and pathophysiological features are different to that of the colon.
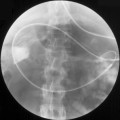
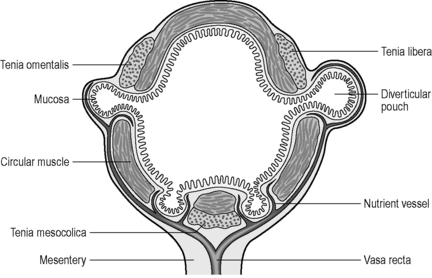
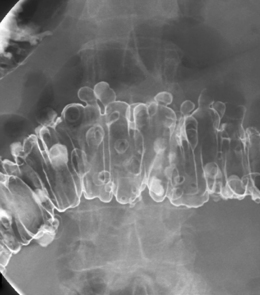
The English physician, Sir David Drummond, described an arterial ring around the colon, the ‘marginal artery of Drummond’ (Gunasekera et al., 2003; Floch and Bina, 2004). The vasa recta arise at frequent intervals around the marginal artery. Dividing at the tenia mesocolica, the vasa recta branches into nutrient vessels that supply the colon. The nutrient vessels pass deep via a canal either side of mesocolica and on the mesenteric side of teniae libera and omentalis (Bassotti et al., 2003; Floch and Bina, 2004). Along these canals the nutrient artery passes through the circular muscle fiber to its origin. In the right circumstances, these canals constitute the weak points through which the mucosa can protrude creating a diverticulum (Figures 15.1 and 15.2).
Pathogenesis
Papers by Painter and Burkitt (1971), Smith (1986), Aldoori et al. (1998), Frieri et al. (2006) and Blackwood and Salter (2000) are among the many that support the hypothesis that dietary fiber reduces the risk of diverticular disease and, conversely, the risk being increased by a lack of fiber, particularly the insoluble fiber hydrocolloid cellulose.
The dietary fiber hydrocolloid cellulose is a non-digestible carbohydrate found in plant material. Although this cellulose itself has a low water content, it is porous and has a significant capability to retain water within its pores. Hydrocolloid cellulose is also resistant to the effects of enzymes in the small bowel and it can provide support for the growth of microflora in the colon as fermentation takes place. It is the high water-retaining capability of the insoluble element of cellulose that is responsible for the (beneficial) formation of a more bulky stool. This results in the maintenance of colonic lumen diameter commensurate with the stool volume. The fluid retained within the stool as a result of dietary fiber intake reduces fecal viscosity and results in a reduced transit time (Prosky and Dreher, 1999; Bassotti et al., 2003). Painter and Burkitt (1971) reported that, in areas of Africa where the population has a high fiber intake, normal colonic transit time was half that common in the West at that time.
Understanding the widely accepted hypothesis as to what provides and constitutes a good stool enables an understanding of the converse, that a lack of dietary fiber results in a reduction in fecal water content. This leads to the stool being more compact and smaller in diameter and with an increased viscosity. The denser less viscous stool, in conjunction with the reduced diameter of the colon, results in a higher intraluminal pressure requirement to pass the fecal column through the bowel. The slower passage of the stool though the colon allows more fluid to be absorbed maintaining the vicious circle that supports the pathogenesis of diverticular disease (Table 15.1).
Table 15.1 Pathogenesis of diverticular disease
| Lack of dietary fiber increases the risk of diverticular disease | |
|---|---|
| High fiber intake | Low fiber intake |