Fig. 3.1
Direct comparison of segmental coronary artery anatomy, as depicted by CT (left panels, three-dimensional reconstructions) and conventional coronary angiography (right panels). If an intermediate branch is present (about 30% of patients) this segmentation model consists of 17 segments. The RCA with its five segments is shown in Panels A and B, and the left coronary artery with its two main branches – the left anterior descending and the left circumflex – in Panels C–F. The RCA (Panels A and B) is composed of segments 1–4, with the distal segment (4) being further subdivided into 4a (posterior descending artery, PDA) and 4b (right posterolateral branch). The left main coronary artery (Panels C–F) is referred to as segment 5, and the left anterior descending coronary artery (Panels C and D) is composed of segments 6–10, with the two diagonal branches being segments 9 and 10. The LCX (Panels E and F) is composed of segments 11–15, with the two (obtuse) marginal branches being segments 12 and 14. Note that the distal left circumflex (segment 15) is rather small in this patient with a right-dominant coronary circulation. The sinus node artery (SN) is the first branch of the LCX in this patient (Panels E and F) but is more commonly one of the first branches of the RCA. AM acute marginal branch, CB conus branch. Table 3.1 gives an overview of all coronary artery segment numbers and names
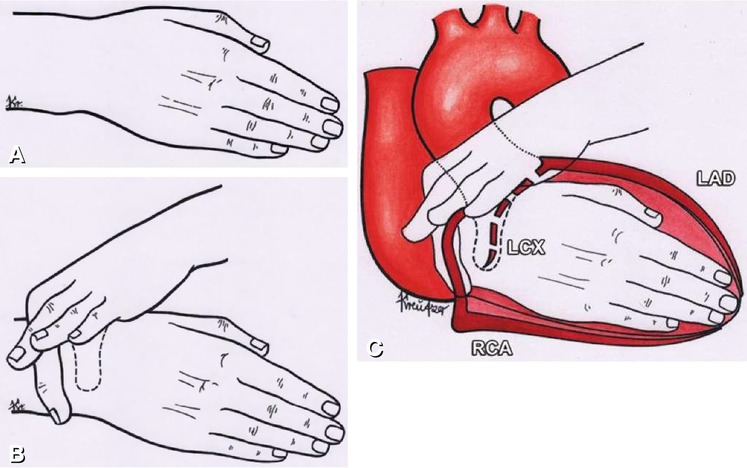
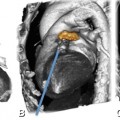
Fig. 3.2
Simple method of teaching three-dimensional coronary artery anatomy. The technique utilizes the concept of two imaginary circles around the interventricular and atrioventricular grooves, which are indicated by the position of the demonstrator’s right and left hand, respectively. Panel A shows the right hand which demonstrates the position of the interventricular septum with its margins, the posterior and anterior interventricular groove. In Panel B the atrioventricular groove is represented by the thumb and index finger of the added left hand, which encircle the right wrist. The superimposed cardiac structures with the coronary arteries are shown in Panel C. LAD left anterior descending artery, LCX left circumflex coronary artery, RCA right coronary artery (Adapted from Sos and Sniderman, Radiology, 1980)
The right coronary artery (RCA) arises from the aorta at the right sinus of Valsalva and courses in the right atrioventricular groove. Along its course, it first gives off the conus artery (in 50% of all individuals; in the other 50%, the conus artery arises directly from the aorta). It then gives off the sinoatrial node artery (in roughly 60%; in the remaining individuals, it arises from the left circumflex coronary artery [LCX]). Acute marginal branches arise from the mid-segment and posterior right ventricular branches from the distal segment. In case of a right-dominant circulation, the RCA gives rise to the posterior descending artery (PDA) at or near the crux cordis (where the left and right atrioventricular groove and posterior interventricular groove join), from where it courses in the posterior interventricular groove, and the RCA gives rise to posterolateral artery branches as it continues in the left atrioventricular groove beyond the crux. In case of a left-dominant circulation, the LCX gives rise to the PDA. The RCA supplies both the myocardium of the right atrium and ventricle and inferior portions of the left ventricle and interventricular septum.
The left main coronary artery (LM) arises from the aorta at the left sinus of Valsalva and has a length that varies from 0 to 15 mm. The LM usually bifurcates into the left anterior descending coronary artery (LAD) and LCX; however, in a third of the population, the LM ends as a trifurcation with an intermediate branch (IMB, also called ramus medianus) arising between the LAD and the LCX (Fig. 3.3). An IMB can be regarded as a diagonal branch or as an obtuse marginal branch, depending on its course along the left ventricle. In about 1% of the population, the LM is absent, and there are separate ostia for the LAD and LCX (Fig. 3.3).
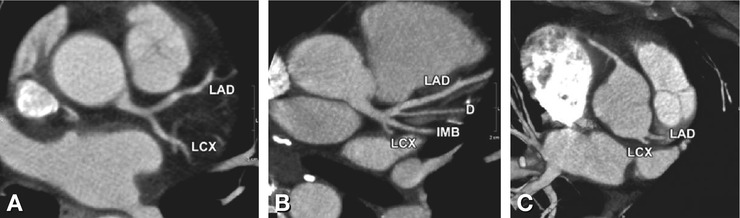
Fig. 3.3
Different types of left main coronary artery bifurcation. Oblique transverse thin-slab maximum-intensity projection images. The left main coronary artery is shown bifurcating into the left anterior descending coronary artery (LAD) and left circumflex coronary artery (LCX, Panel A), the left main with trifurcation into the LAD and the LCX, and in between an intermediate branch (IMB, Panel B). Note the high diagonal branch (D) from the LAD (Panel B). An absent left main coronary artery, with separate origins for the LAD and LCX (Panel C)
The LAD courses in the anterior interventricular groove. The major branches of the LAD are the septal branches that pass downward into the interventricular septum and the diagonal branches (usually one to three are present) that pass over the anterolateral aspect of the heart. The LAD and its side branches supply the anterior as well as the anteroseptal and anterolateral left ventricular segments. The septal branches, in particular, serve as important collateral pathways.
The LCX courses in the left atrioventricular groove, where the major side branches are the obtuse marginal branches (usually one to three are present) that supply the lateral free wall of the left ventricle. The left atrial circumflex branches that supply the lateral and posterior aspect of the left atrium also arise from the LCX.
3.1.1 Coronary Artery Dominance
The circulation is right-dominant in about 60–85% of the population (the RCA gives rise to the posterior descending and at least one posterolateral branch). Left coronary dominance (the LCX gives rise to the PDA) is found in 7–20% of the population, whereas a balanced (or co-dominant) distribution is seen in 7–20% (the RCA gives rise to the PDA, and the LCX gives rise to posterolateral branches). In the case of a left-dominant circulation, the RCA is small and does not supply blood to the left ventricular myocardium. Recognizing the dominancy of the circulation is important, so as to avoid confusing this situation with branch occlusion (e.g., a short RCA in a left-dominant circulation, Fig. 3.4). Although it is the RCA that is typically dominant, it is usually the left coronary artery that supplies the major part of the left ventricular myocardium as well as the anterior and mid portions of the interventricular septum.
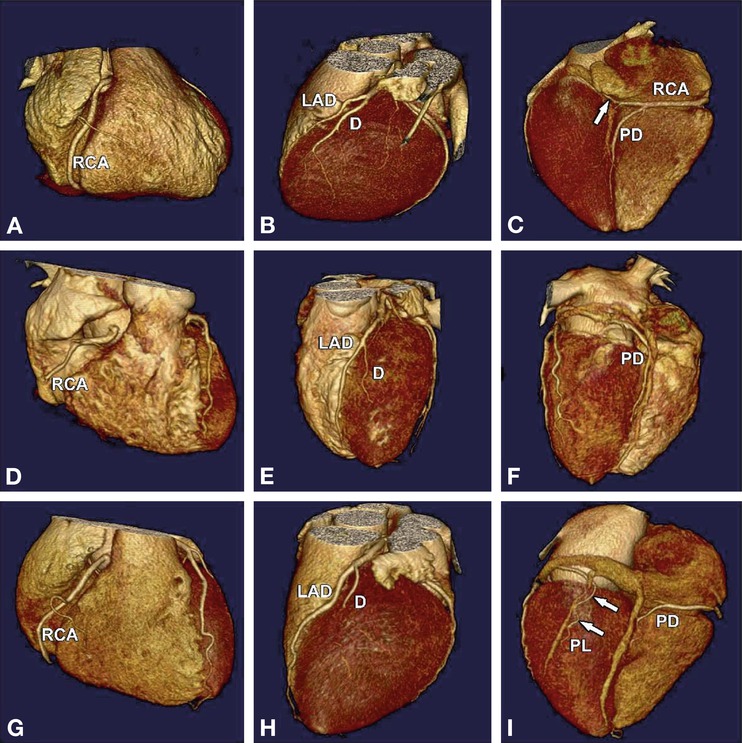
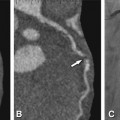
Fig. 3.4
Different coronary artery distribution types on three-dimensional volume-rendered images. Panels A–C: Right-dominant circulation. The RCA is dominant and gives rise to the posterior descending artery (PD), and also continues in the left atrioventricular groove (arrow in Panel C). Panels D–F: Left-dominant circulation. The LCX is dominant and gives rise to the posterior descending artery (PD in Panel F). Note the small RCA in the left-dominant coronary artery system (Panel D). Panels G–I: Balanced circulation (codominant circulation), where the RCA gives rise to the PD and the LCX gives rise to a posterolateral branch (PL in Panel I). D diagonal branch; LAD left anterior descending artery
3.1.2 Coronary Artery Segments
The coronary arteries with their side branches can be further subdivided and classified (Figs. 3.1, 3.5, 3.6, and 3.7 and Table 3.1). These segments are of importance in describing the location of significant coronary stenoses found on noninvasive imaging and correlating them with possible myocardial ischemia, as well as for accurately guiding subsequent revascularization. Use of the 17-segment model further described in Table 3.1 and Figs. 3.1, 3.5, 3.6, and 3.7 is recommended for this purpose; in the case of pathology (i.e., the presence of stenoses), it is recommended that the location be reported either by segment name or by number. The 17-segment model has advantages over its competitor segmentation schemes, the foremost being its simplicity and conciseness.
Get Clinical Tree app for offline access
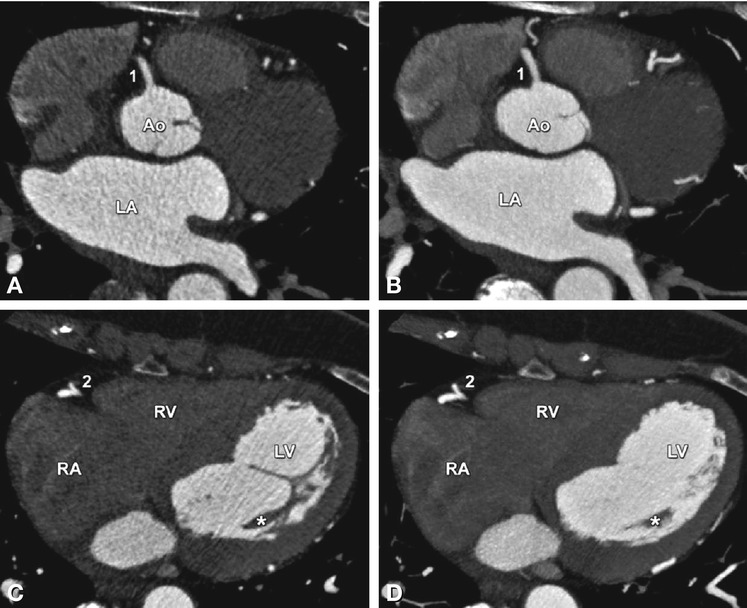
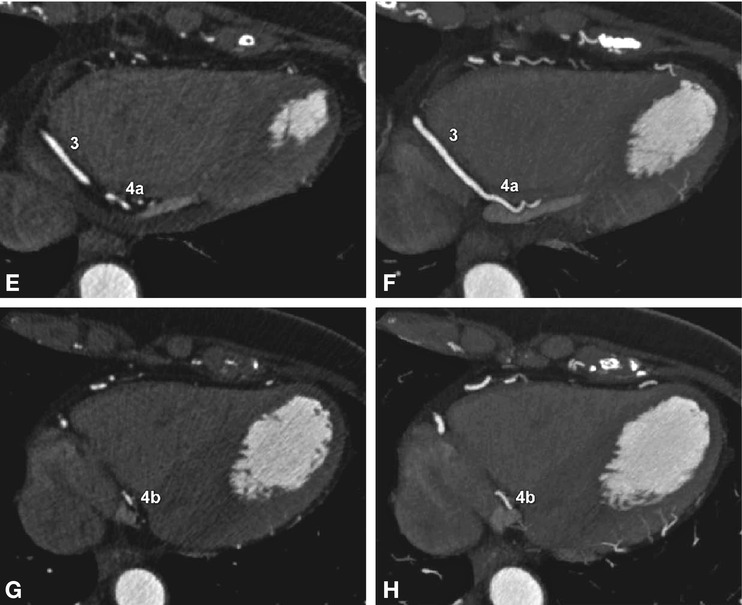
Fig. 3.5
The RCA with all its segments in axial slices (left panels), and the corresponding maximum-intensity projections of 5-mm thickness in the axial orientation for comparison (right panels). The proximal segment of the RCA (1) comes off the aorta, arising from the right sinus of Valsalva (Panels A and B). It first moves anteriorly and then (as segment 2) caudally in the right atrioventricular sulcus (Panels C and D) to the posterior surface of the heart (Panels E and F) where it again moves in the horizontal plane on the diaphragmatic face of the heart as segment 3. At the crux cordis, segment 3 bifurcates into the posterior descending artery (4a) and the right posterolateral branch (4b in Panels G and H). In cases of dominance of the RCA (as in this case), segments 4a and b are side branches of the RCA. In case of left coronary artery dominance, the posterior descending artery (4a) is part of the LCX. Ao aorta, Asterisk papillary muscles, LA left atrium, LV left ventricle, RA right atrium, RV right ventricle
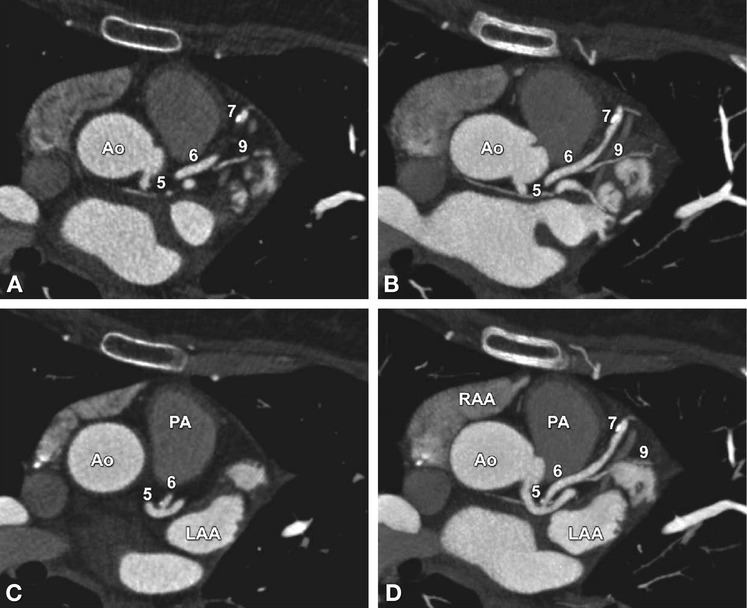
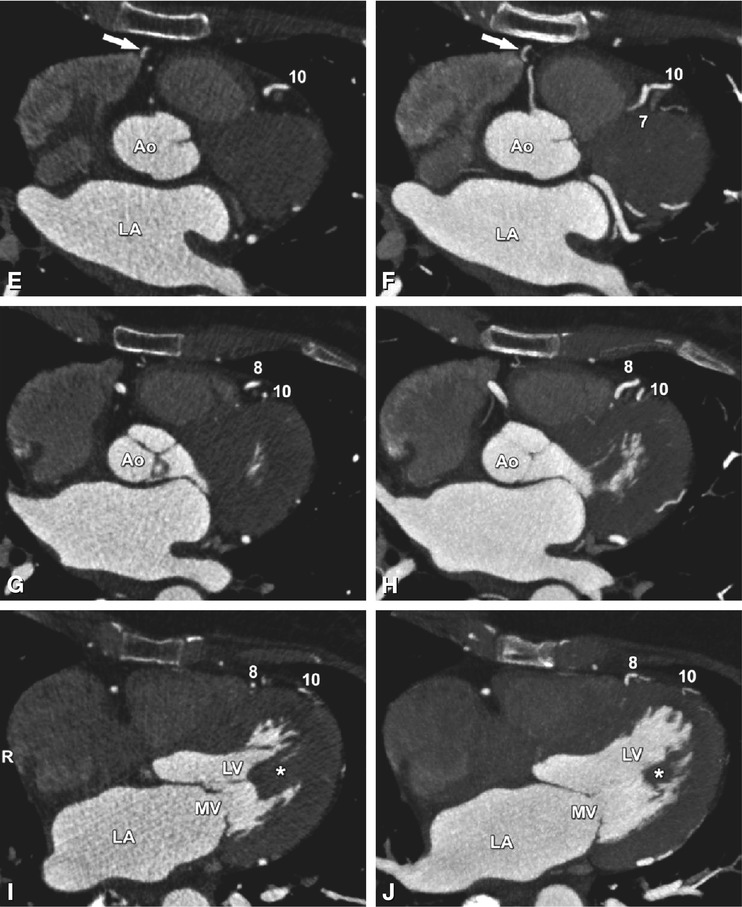
Fig. 3.6
The left anterior descending coronary artery with all its segments in axial slices (left panels), and the corresponding maximum-intensity projections of 5-mm thickness in the axial orientation for comparison (right panels). The proximal left anterior descending coronary artery segment (6) is the anterior branch of the left main coronary artery (5, Panels A–D




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
