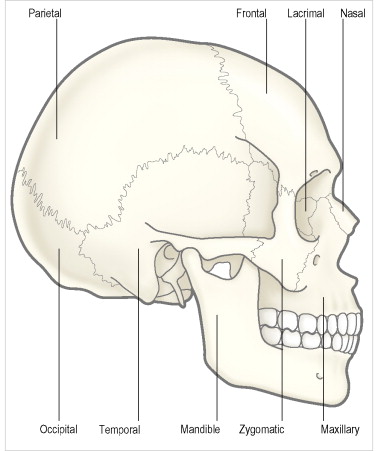
The skull is composed of two segments, the cranium and the face. The cranium is the major portion and it consists of three unpaired bones, the sphenoid, occipital, and ethmoid bones, and three paired bones, the frontal, parietal, and temporal bones. The face is attached anteriorly and consists of two unpaired bones, the vomer and mandibular bones, and six paired bones, the nasal, maxillary, zygomatic, palatine, lacrimal, and inferior turbinate bones. The orbit is made up of portions of both the cranial and the facial skeletal systems.
The cranium
Sphenoid bone
The base of the skull is formed primarily by the unpaired sphenoid and occipital bones ( Figure 3.1 ). Posteriorly the body of the sphenoid bone abuts the occipital bone, and anteriorly it articulates with the ethmoid bone centrally and with the frontal bones just lateral to the midline. More inferiorly the anterior sphenoid contacts the maxillary and palatine bones. A small depression is located on the intra-cranial surface of the sphenoid body, the sella turcica or pituitary fossa. It is bounded anteriorly by paired elevated ridges called the anterior clinoid processes, and posteriorly by a horizontal raised ridge, the posterior clinoid process. The central portion of the sphenoid bone is a hollow cavity, the sphenoid sinus.

From the body of the sphenoid bone two pairs of thin plates extend laterally. The lesser wings of the sphenoid bone, one on either side, arise as a narrow strut from the sphenoid body and project superiorly and laterally to articulate along their anterior surface with the ethmoid bone centrally and with the frontal bones. The small canal that is formed between the body and lesser wing of the sphenoid is the optic canal. The greater wings of the sphenoid bone arise from the body and project laterally. They articulate with the frontal bones anteriorly, the temporal and parietal bones posterolaterally, and the zygomatic bones anterolaterally. Inferiorly, the small pterygoid process projects downward from the greater wing near its base, where it joins the palatine bone to form the lateral wall of the pterygopalatine fossa. The latter communicates with the orbit via the inferior orbital fissure. The longitudinal space between the greater and lesser sphenoid wings is the superior orbital fissure, a major conduit between the middle cranial fossa and the posterior orbit.
Three additional foramina are found in the greater wing. The foramen rotundum lies anterior between the body of the sphenoid and the root of the greater wing, and transmits the maxillary branch of the trigeminal nerve (V 2 ). The foramen ovale is slightly larger and more posterior on the greater wing, and transmits the mandibular branch of the trigeminal nerve (V 3 ). The foramen spinosum is located near the posterior edge of the greater wing and carries a branch of the middle meningeal artery and the recurrent branch of the mandibular nerve (V 3 ).
Occipital bone
The occipital bone forms the posterior portion of the posterior cranial fossa and the posterior segment of the skull base ( Figure 3.2 ). It has a large opening on its inferior surface, the foramen magnum, through which the spinal cord passes. The base of the occipital bone articulates anteriorly with the body of the sphenoid bone. Superiorly it joins the parietal bones along a complex suture line, and laterally it articulates with the temporal bones. A strong roughly horizontal ridge runs along the back of the occipital bone onto which the occipital muscle inserts.
Temporal bone
The temporal bones form the lateral portions of the middle cranial fossa and the anterior portion of the posterior cranial fossa ( Figure 3.2 ). The wing-like squamous portion of this bone articulates superiorly with the parietal bone and anteriorly with the greater wing of the sphenoid. Posteriorly and inferiorly is a thickened pyramidal structure called the petrous portion of the temporal bone. This joins the occipital bone along the cranial base and houses the middle and inner ear. Externally, the external auditory canal forms the entrance into this structure. The protuberance of bone immediately posterior to the canal is called the mastoid process. Just medial to the mastoid is a slender projection of bone, the styloid process, which lengthens with age and serves as the origin for the stylopharyngeal, stylohyoideus, and styloglossus muscles. Between the mastoid and styloid process is the stylomastoid foramen, through which passes the facial nerve as it exits the cranial cavity.
Frontal bone
The frontal bone in the adult is an unpaired structure forming the anterior portion of the cranial cavity ( Figure 3.3 ). Externally, it contributes to the facial skeleton where it represents the forehead and supraorbital ridges. The frontal bone joins the parietal bones superiorly, and inferiorly it articulates with the sphenoid, ethmoid, and lacrimal bones in the orbit. Anteriorly the frontal joins the frontal process of the maxillary bone and the nasal bone at a short suture between the orbits. Laterally, the frontal forms a short suture with the zygomatic bone at the superolateral portion of the orbital rim. Within the anterior portion of the frontal bone behind the supraorbital ridges are the paired frontal sinuses.

Ethmoid bone
The ethmoid bone is an unpaired structure in the midline ( Figure 3.4 ). Superiorly a perforated plate of bone, the cribriform plate, forms the floor of the anterior cranial fossa between the frontal and sphenoid bones. These perforations transmit fibers of the first cranial or olfactory nerve into the nose. A central vertical septum divides the ethmoid into a left and right half, each containing numerous air cells. Laterally, a thin plate of bone, the lamina papyracea forms the medial wall of the orbit. The ethmoid bone articulates with the frontal bone superiorly, the sphenoid bone posteriorly, the lacrimal bone anteriorly, and the maxillary bone inferiorly.

Nasal bone
The nasal bones are paired plates that form the bridge of the nose in the central part of the face ( Figures 3.2 and 3.3 ). They articulate with each other in the midline, with the frontal bone superiorly, and with the frontal process of the maxillary bone inferiorly. Although they do not contribute to the cranial cavity or the orbit, the nasal bones are important as they are frequently involved in pathology and trauma in the adjacent orbit.
The orbit
Bones of the orbit
The bony orbit forms from the mesenchyme that encircles the optic vesicle beginning as early as the 6-week embryonic stage. Individual bones develop from a complex series of primary or secondary ossifications around the evolving optic cup and stalk. Initially, the optic vesicles are positioned 170–180° apart, on opposite sides of the forebrain. Later these begin to rotate anteriorly as the primordial orbital bones are laid down around them.
In the adult, the bony orbit encloses a volume of about 30 cm 3 . It is composed of seven bones ( Figure 3.4 ), simplified from a complex of dermal and endochondral elements of earlier vertebrates. Except for a series of canals, fissures, and foramina that communicate with extraorbital compartments, the orbit is a closed space with a broad opening anteriorly. This explains the frequent development of proptosis as a clinical sign even in early stages of orbital disease.
The orbital roof
The orbital roof is composed of the orbital plate of the frontal bone with a small contribution from the lesser wing of the sphenoid at the apex ( Figures 3.4 and 3.5 ). It is a thin lamina separating the orbit anteriorly from the frontal sinus, and posteriorly from the anterior cranial fossa. The roof slopes backward and downward toward the apex, where it ends at the optic canal and superior orbital fissure. The canal assumes a vertically oval shape at its orbital end, where it measures about 5–6 mm in diameter. It is 8–12 mm in length, and is oriented posteromedially about 35° to the mid-sagittal plane, and upward about 38° to the horizontal.

The lateral orbital wall
The lateral wall is formed by the greater wing of the sphenoid bone posteriorly, and by the zygomatic process of the frontal bone and the orbital process of the zygomatic bone anteriorly. It lies at a nearly 45° angle to the mid-sagittal plane. The lateral wall is bounded below by the inferior orbital fissure, and medially by the superior orbital fissure. Behind the thick lateral orbital rim, the wall becomes quite thin where the zygomatic bone joins the greater sphenoid wing at a vertical suture line. During a lateral orbitotomy, cutting the rim through to this thin plate allows easy outward fracture of the bone. The convoluted frontozygomatic suture line runs approximately horizontally and crosses the superotemporal rim near the lacrimal gland fossa. About 5–15 mm above this line, the frontal bone widens as it passes around the front end of the anterior cranial fossa. The surgeon must take note of this broadening contour in planning the position of the superior bone cut in a lateral orbitotomy. About halfway along the lateral wall, in the sphenoid wing near the frontosphenoid suture, is a small canal carrying an anastomotic branch between the lacrimal and meningeal arteries. Elevation of the periorbita during lateral orbital dissection may result in brisk bleeding from this vessel, but this is usually easily controlled with pressure. Just behind the zygomaticosphenoid suture line, the greater wing widens as it passes around the anterior tip of the middle cranial fossa. As the greater wing is removed during lateral orbitotomy procedures, the appearance of cancellous bone warns of the imminent approach of dura.
The orbital floor
The floor is the shortest of the orbital walls, extending back only about 35–40 mm from the inferior rim. The orbital floor is composed primarily of the maxillary bone, with the zygomatic bone forming the anterolateral portion, and the palatine bone lying at the posterior extent of the floor. Its surface forms a triangular segment extending from the maxillary-ethmoid buttress, horizontally to the inferior orbital fissure, and from the orbital rim back to the posterior wall of the maxillary sinus. The floor ends at the posterior limit of the maxillary sinus and, therefore, does not extend to the orbital apex. The orbital floor is thinnest just medial to the infraorbital canal and this is the most common site for blow-out fractures. Despite its thinness, the floor is strengthened by the infraorbital canal, which runs through it near its center, and by the presence of one or more trabeculae in the roof of the maxillary sinus. Nevertheless, the orbital floor shows the greatest degree of deformation with external force of any of the orbital walls. This explains the high rate of floor fractures associated with even minor blunt trauma.
The infraorbital groove begins at the inferior orbital fissure and runs forward in the maxillary bone. About 15 mm from the orbital rim, this groove usually becomes bridged over with a thin lamina of bone to form the infraorbital canal. Within this canal runs the maxillary division of the trigeminal nerve with the maxillary artery. These structures exit just below the central orbital rim at the infraorbital foramen. Surgery on the orbital floor during blow-out fracture repair or orbital decompression must pay special attention to these structures to avoid injury.
Separating the floor from the lateral orbital wall is the inferior orbital fissure. This opening is approximately 20 mm in length, and runs in an anterolateral to posteromedial direction. At the orbital apex just below the optic canal, the inferior fissure joins the superior orbital fissure, and is contiguous with the foramen rotundum. The inferior fissure transmits structures into the orbit from the pterygopalatine fossa posteriorly, and from the infratemporal fossa anteriorly. Multiple branches from the inferior ophthalmic vein pass through this opening to communicate with the pterygoid venous plexus. The inferior fissure also transmits the maxillary division of the trigeminal nerve from the foramen rotundum to the infraorbital sulcus along the orbital floor, where it runs in company with the infraorbital artery. Postganglionic parasympathetic secretory and vasomotor neural branches from the pterygopalatine ganglion enter the orbit through the inferior orbital fissure, where they join with the maxillary nerve for a short distance before passing to the lacrimal gland.
The medial orbital wall
The medial walls of the orbits are approximately parallel to each other and to the mid-sagittal plane. The medial wall is composed largely of the lamina papyracea of the ethmoid bone ( Figure 3.4 ). This thin plate is exceptionally fragile, measuring only 0.2–0.4 mm in thickness, and separates the orbit from air cells of the ethmoid sinus labyrinth. It is a frequent site of fracture in orbital trauma, and is easily breached during transnasal ethmoid sinus surgery. The lamina papyracea offers little resistance to expanding ethmoid sinus mucoceles, and commonly transmits inflammatory and infectious processes from sinusitis into the orbit.
Posterior to the ethmoid, the body of the sphenoid bone completes the medial wall to the apex. This portion of the wall is quite thick and is only rarely involved in orbital trauma or sinus pathology. The medial wall ends at the optic foramen where the sphenoid forms the medial wall of the optic canal.
Anterior to the ethmoid is the lacrimal bone, a thin plate containing the posterior lacrimal crest, and forming the posterior half of the lacrimal sac fossa. In the mid portion of the fossa the lacrimal bone joins the orbital process of the maxillary bone at a vertical suture line. The latter is a thick bone that forms the medial orbital rim. During lacrimal bypass surgery, entrance into the nose can be achieved easily with a hemostat by applying gentle pressure on the lacrimal portion of the fossa. In some individuals the lacrimal bone is situated further posterior so that the maxillary bone underlies most of the fossa. In such cases, a burr is necessary to remove enough bone to create a lacrimal–nasal ostium.
Within the frontoethmoid suture line in the superomedial orbit are two openings, the anterior and posterior ethmoidal foramina. The former usually lies 20–25 mm behind the anterior lacrimal crest, and the latter about 32–35 mm behind the anterior crest and 5–10 mm anterior to the optic canal. These foramina transmit branches of the ophthalmic artery and nasociliary nerve into the ethmoid sinus and nose. The ophthalmic artery branches are frequently injured in orbital trauma, and are the major sources of subperiosteal hematomas. During surgery on the medial orbital wall, the position of these foramina must be kept in mind to avoid injury and hemorrhage. In addition, these openings mark the approximate level of the roof of the ethmoid labyrinth, and the floor of the anterior cranial fossa. The cribriform plate may lie up to 10 mm below this level just medial the root of the middle turbinate, and can be fractured during medial wall surgery.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


