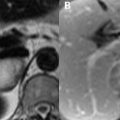
12 Aneurysms Aneurysms are the most common cause of SAH and a frequent cause of intraparenchymal hemorrhage, the imaging features of which were described in previous chapters. Non-ruptured aneurysms are usually asymptomatic, but may cause mass effect or produce emboli from areas of partial thrombosis. Risk factors include smoking and binge drinking, along with collagen vascular, connective tissue, and polycystic kidney diseases. Intracranial aneurysms frequently occur in the feeding arteries of AVMs, presumably from increased flow. Aneurysms are broadly classified into fusiform (spindle-shaped) and saccular (spherical) types. Fusiform aneurysms frequently occur secondary to arteriosclerosis and favor the basilar and intracranial carotid arteries. Saccular or berry aneurysms are far more common and result from a congenital defect in the tunica media. These aneurysms involve, in decreasing frequency, the anterior communicating (Fig. 12.1A, white arrow), posterior communicating (Figs. 12.1B,C, white arrows), and middle cerebral arteries (MCAs). MCA involvement frequently occurs at the bifurcation or trifurcation. Flow dynamics at arterial branch points render these favorable locations for aneurysm development. MRI is the noninvasive screening test of choice for the detection and evaluation of intracranial aneurysms. TOF MRA is the specific sequence of choice, with maximum intensity projection (MIP; Figs. 12.1A,B,F) or volume rendering (Fig. 12.1C
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


