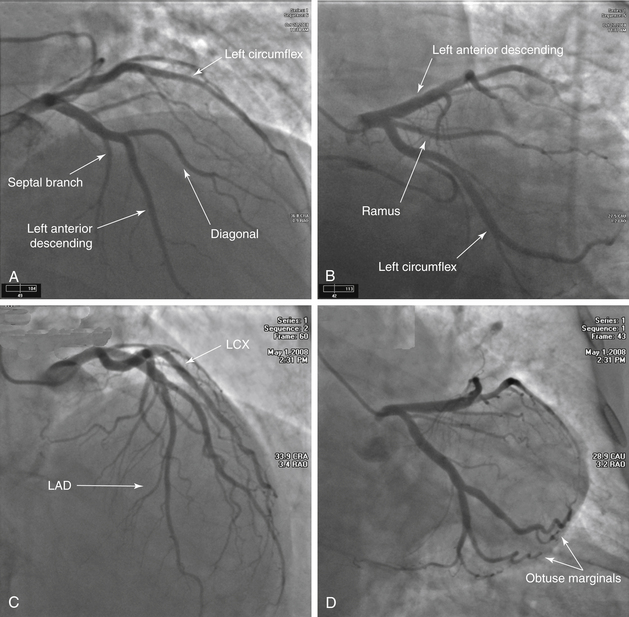
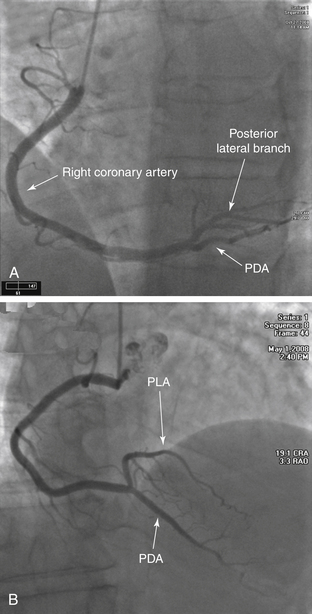
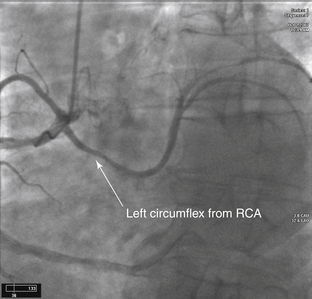
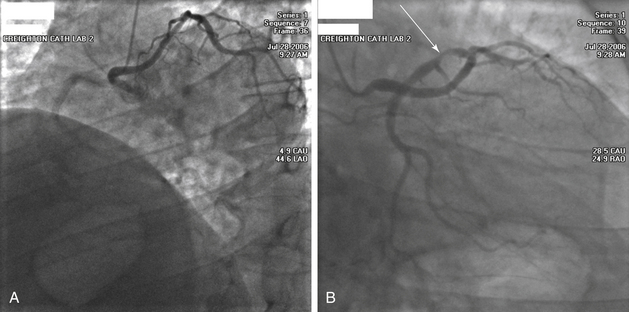
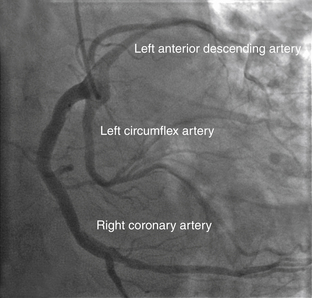
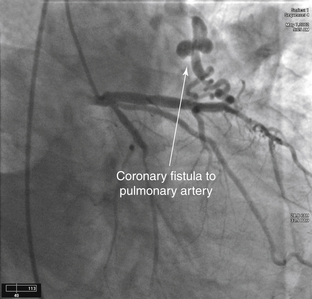
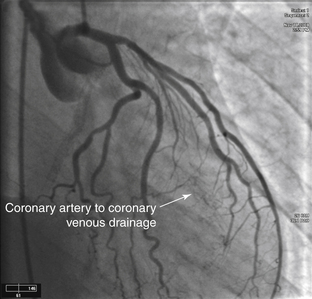
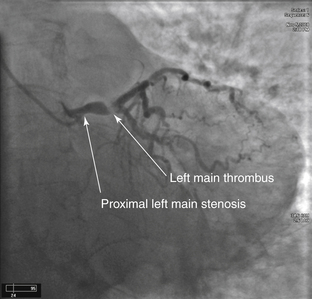
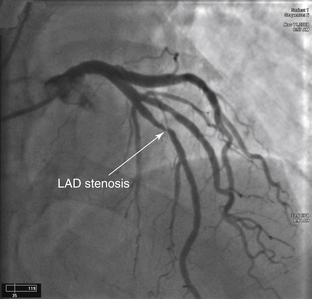
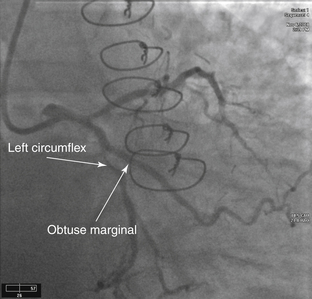
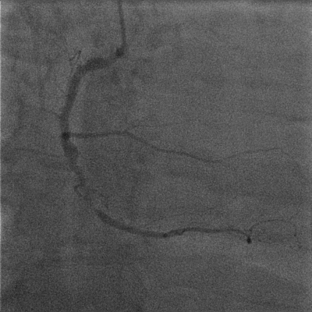
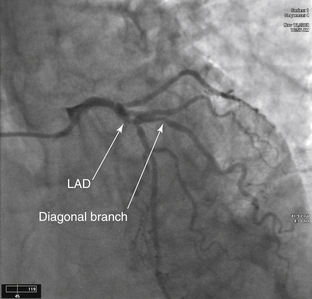
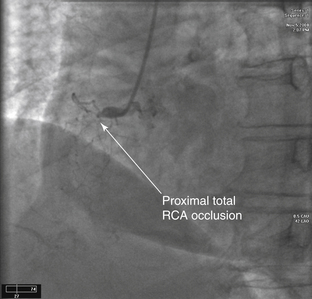
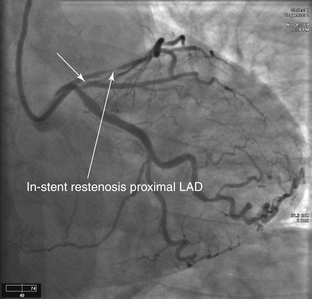
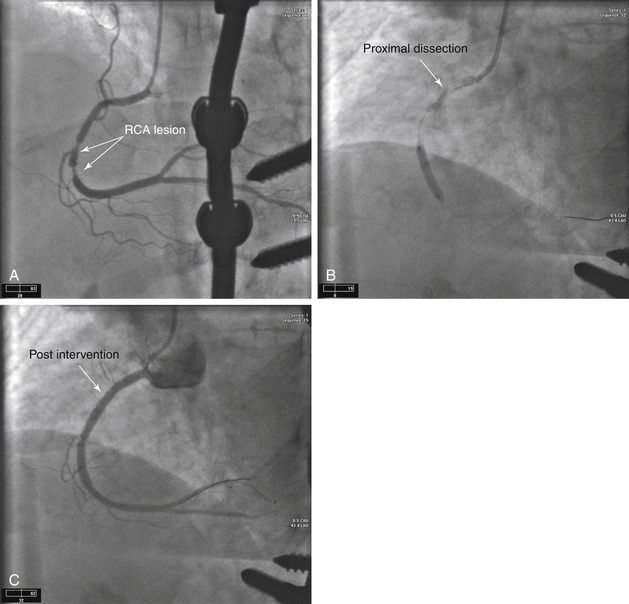
3 Angiography FIGURE 3-1 Left coronary system. A, A Judkins left 3.5 catheter has been advanced to the LMCA ostium via the right radial approach. This projection is obtained in the AP cranial view. The LMCA arises in the normal location from the left sinus of Valsalva. The LAD travels down toward the bottom of the image. The major branches that arise from this artery are the septal penetrators and the diagonals. The LCX is located across the top of the image and moves toward the right. This view has significant overlap of the circumflex branches, noted by the double density of contrast media. B, The AP caudal projection demonstrates the bifurcation of the LAD and LCX systems and is used to look for ostial stenoses. The LCX gives rise to major branches that are termed obtuse marginals. In this image, a branch occurs between the LAD and LCX, arising from the LMCA. When present, the artery is named the ramus intermediate. C, An AP cranial view of another normal LAD. This image allows better visualization of the mid- and distal LAD. In this patient, the first diagonal is nearly the same size as the LAD. D, Finally, another AP caudal projection demonstrating the bifurcation of the LAD and LCX systems. There is no significant CAD present in this patient. The LCX system is seen as it travels toward the bottom right corner of this image. The LAD is located at the top of the image moving horizontally across. FIGURE 3-2 Right coronary system. A, A Judkins right 4.0 catheter is placed at the ostium of the RCA, and an angiogram is obtained in the straight LAO projection. No significant disease is noted. This is a right dominant coronary system; the PDA arises from the distal RCA. B, This is an AP cranial view of another RCA. The bifurcation of the posterior descending coronary artery and posterolateral coronary artery is best visualized in this view. FIGURE 3-3 Anomalous LCX. Diagnostic cardiac catheterization in a patient with unstable angina. The LCX arises off the right coronary cusp from the same orifice as the RCA (anomalous origin of the LCX). The most common coronary anomaly is separate ostia of the LCX and LAD arising from the left sinus of Valsalva. This is followed by the LCX arising from the RCA or right sinus of Valsalva. Most coronary anomalies are clinically silent; however, if the LMCA arises from the pulmonary trunk or aberrantly courses between the great vessels, an increased association with sudden death, myocardial ischemia, and endocarditis is seen. FIGURE 3-4 Anomalous left main from the right coronary cusp. A, This image is obtained in the LAO projection. A Judkins right catheter has been advanced into the aorta from the right radial artery. As contrast medium is injected, there is faint filling of the RCA coming toward the left side of the image. The catheter, however, is in the ostium of the LMCA. The LMCA is anomalous and transverses across the heart muscle and bifurcates into the LAD and LCX. In this view, it appears that the artery courses anterior to the aorta, but further imaging should be performed to confirm this positioning. B, This image is obtained in the RAO projection. This clearly demonstrates that the LMCA is very long and extends to the left ventricular side before it bifurcates. There is severe stenosis of the proximal LCX (arrow). FIGURE 3-5 Single coronary artery. A Judkins right 4.0 coronary catheter is noted in the right coronary cusp on this LAO projection. As the contrast enters the artery, all three of the major coronary arteries are visualized arising from the same common trunk. The RCA follows the standard course toward the inferior border of the heart. The LCX is located in the middle of the image and travels to the lateral wall of the ventricle. The LAD is toward the back of the image and is recognized secondary to the presence of septal branches. This anomaly is rare, occurring in 0.02% of the population. FIGURE 3-6 Coronary artery fistula. LAO view of the left coronary system during diagnostic catheterization. Note the fistula from the LAD to the PA. This is the most common type of coronary artery fistula. Other connections include from a coronary artery to the right ventricle, right atrium, or coronary sinus. FIGURE 3-7 Coronary artery to coronary venous drainage. A Judkins left 4.0 catheter has been placed in the ostium of the LMCA via the femoral approach. The angiogram is obtained in the RAO caudal projection. As the contrast medium enters the left coronary circulation, staining is noted in the middle of the cardiac silhouette that partially clears with ventricular systole. This is consistent with coronary artery to coronary venous drainage. The coronary venous drainage occurs through the thebesian system directly into the ventricles. FIGURE 3-8 Left main stenosis with thrombus. A Judkins left 3.5 catheter is placed in the LMCA ostium from the right radial approach. In the AP caudal projection, a lesion is noted at the origin of the LMCA. Comparing the diameter of the vessel proximal to and distal to the lesion, a significant narrowing is noted. The most striking portion of this angiogram is the hazy lucent portion of the artery at the bifurcation of the LAD and LCX, secondary to a large thrombus. In the cine angiograms, the flow into the distal vessels is slightly impaired. An additional thrombus is noted in the mid-LCX. In addition, the RCA is filled late by collaterals, demonstrating that the proximal portion of the artery is likely occluded. The entire coronary circulation is compromised by the thrombus. FIGURE 3-9 Left anterior descending artery stenosis. A Judkins left coronary catheter is positioned in the LMCA ostium from the right radial approach. The camera is positioned in the AP cranial projection. In the middle of the frame, a significant flow-limiting stenosis is seen in the mid-LAD. This lesion is located after the bifurcation of the first diagonal branch. Comparing the luminal diameter in the arterial segment proximal to and distal to the lesion, there is an approximate 90% to 99% narrowing of the artery. FIGURE 3-10 Left circumflex artery stenosis. This angiogram is obtained via the radial approach in the LAO caudal projection. This view is ideal for separating the ostia of the LAD and LCX. The LAD is the more superior vessel and travels to the left of the image. The LCX is the lower vessel and travels toward the bottom of the image. A 90% to 99% lesion is present in the midportion of the LCX just after the takeoff of the first obtuse marginal branch. The area appears to be slightly more radiolucent than the surrounding vessel. This is an irregular plaque producing significant narrowing. FIGURE 3-11 Right coronary artery stenosis. This angiogram of the RCA is obtained in the straight LAO projection. A severe obstructive lesion is seen in the midsegment of the vessel. The segment of artery distal to the large acute marginal branch is diseased as it enters the area with the severe lesion. The distal vessel is small but relatively free of disease. FIGURE 3-12 Left anterior descending/diagonal stenosis. The image has been obtained in the AP cranial projection. In the middle of the frame, a significant stenosis of the LAD involving the bifurcation of a large diagonal branch is seen. This stenosis makes percutaneous intervention more complicated because there is a risk that flow will be compromised within this side branch. FIGURE 3-13 Total right coronary artery occlusion. A Judkins right 4.0 catheter is positioned at the ostium of the RCA. This image is obtained in the LAO view. The artery is totally occluded proximally. The lesion is said to be in the proximal portion of the vessel because it occurs before the first major acute marginal branch. The mid-RCA is defined as the portion of the artery from the end of the proximal segment to the next major acute marginal branch. The distal RCA is located from the end of the midsegment to the bifurcation of the PDA. FIGURE 3-14 In-stent restenosis of left anterior descending artery. An XB guiding catheter is present in the LMCA ostium from the radial artery approach. This image was obtained in the AP caudal projection. Before contrast injection, a stent can be visualized in the proximal portion of the LAD. A significant narrowing within the stent is consistent with in-stent restenosis. The LCX is without significant disease. However, there is a significant ostial lesion (short arrow) of the first obtuse marginal branch. FIGURE 3-15 Right coronary artery stenosis with catheter dissection. Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Computed Tomography Cardiovascular Magnetic Resonance Imaging Echocardiography Electrocardiography Cardiovascular Magnetic Resonance Imaging Positioning Occupational Lung Diseases Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Angiography Full access? Get Clinical Tree
3 Angiography FIGURE 3-1 Left coronary system. A, A Judkins left 3.5 catheter has been advanced to the LMCA ostium via the right radial approach. This projection is obtained in the AP cranial view. The LMCA arises in the normal location from the left sinus of Valsalva. The LAD travels down toward the bottom of the image. The major branches that arise from this artery are the septal penetrators and the diagonals. The LCX is located across the top of the image and moves toward the right. This view has significant overlap of the circumflex branches, noted by the double density of contrast media. B, The AP caudal projection demonstrates the bifurcation of the LAD and LCX systems and is used to look for ostial stenoses. The LCX gives rise to major branches that are termed obtuse marginals. In this image, a branch occurs between the LAD and LCX, arising from the LMCA. When present, the artery is named the ramus intermediate. C, An AP cranial view of another normal LAD. This image allows better visualization of the mid- and distal LAD. In this patient, the first diagonal is nearly the same size as the LAD. D, Finally, another AP caudal projection demonstrating the bifurcation of the LAD and LCX systems. There is no significant CAD present in this patient. The LCX system is seen as it travels toward the bottom right corner of this image. The LAD is located at the top of the image moving horizontally across. FIGURE 3-2 Right coronary system. A, A Judkins right 4.0 catheter is placed at the ostium of the RCA, and an angiogram is obtained in the straight LAO projection. No significant disease is noted. This is a right dominant coronary system; the PDA arises from the distal RCA. B, This is an AP cranial view of another RCA. The bifurcation of the posterior descending coronary artery and posterolateral coronary artery is best visualized in this view. FIGURE 3-3 Anomalous LCX. Diagnostic cardiac catheterization in a patient with unstable angina. The LCX arises off the right coronary cusp from the same orifice as the RCA (anomalous origin of the LCX). The most common coronary anomaly is separate ostia of the LCX and LAD arising from the left sinus of Valsalva. This is followed by the LCX arising from the RCA or right sinus of Valsalva. Most coronary anomalies are clinically silent; however, if the LMCA arises from the pulmonary trunk or aberrantly courses between the great vessels, an increased association with sudden death, myocardial ischemia, and endocarditis is seen. FIGURE 3-4 Anomalous left main from the right coronary cusp. A, This image is obtained in the LAO projection. A Judkins right catheter has been advanced into the aorta from the right radial artery. As contrast medium is injected, there is faint filling of the RCA coming toward the left side of the image. The catheter, however, is in the ostium of the LMCA. The LMCA is anomalous and transverses across the heart muscle and bifurcates into the LAD and LCX. In this view, it appears that the artery courses anterior to the aorta, but further imaging should be performed to confirm this positioning. B, This image is obtained in the RAO projection. This clearly demonstrates that the LMCA is very long and extends to the left ventricular side before it bifurcates. There is severe stenosis of the proximal LCX (arrow). FIGURE 3-5 Single coronary artery. A Judkins right 4.0 coronary catheter is noted in the right coronary cusp on this LAO projection. As the contrast enters the artery, all three of the major coronary arteries are visualized arising from the same common trunk. The RCA follows the standard course toward the inferior border of the heart. The LCX is located in the middle of the image and travels to the lateral wall of the ventricle. The LAD is toward the back of the image and is recognized secondary to the presence of septal branches. This anomaly is rare, occurring in 0.02% of the population. FIGURE 3-6 Coronary artery fistula. LAO view of the left coronary system during diagnostic catheterization. Note the fistula from the LAD to the PA. This is the most common type of coronary artery fistula. Other connections include from a coronary artery to the right ventricle, right atrium, or coronary sinus. FIGURE 3-7 Coronary artery to coronary venous drainage. A Judkins left 4.0 catheter has been placed in the ostium of the LMCA via the femoral approach. The angiogram is obtained in the RAO caudal projection. As the contrast medium enters the left coronary circulation, staining is noted in the middle of the cardiac silhouette that partially clears with ventricular systole. This is consistent with coronary artery to coronary venous drainage. The coronary venous drainage occurs through the thebesian system directly into the ventricles. FIGURE 3-8 Left main stenosis with thrombus. A Judkins left 3.5 catheter is placed in the LMCA ostium from the right radial approach. In the AP caudal projection, a lesion is noted at the origin of the LMCA. Comparing the diameter of the vessel proximal to and distal to the lesion, a significant narrowing is noted. The most striking portion of this angiogram is the hazy lucent portion of the artery at the bifurcation of the LAD and LCX, secondary to a large thrombus. In the cine angiograms, the flow into the distal vessels is slightly impaired. An additional thrombus is noted in the mid-LCX. In addition, the RCA is filled late by collaterals, demonstrating that the proximal portion of the artery is likely occluded. The entire coronary circulation is compromised by the thrombus. FIGURE 3-9 Left anterior descending artery stenosis. A Judkins left coronary catheter is positioned in the LMCA ostium from the right radial approach. The camera is positioned in the AP cranial projection. In the middle of the frame, a significant flow-limiting stenosis is seen in the mid-LAD. This lesion is located after the bifurcation of the first diagonal branch. Comparing the luminal diameter in the arterial segment proximal to and distal to the lesion, there is an approximate 90% to 99% narrowing of the artery. FIGURE 3-10 Left circumflex artery stenosis. This angiogram is obtained via the radial approach in the LAO caudal projection. This view is ideal for separating the ostia of the LAD and LCX. The LAD is the more superior vessel and travels to the left of the image. The LCX is the lower vessel and travels toward the bottom of the image. A 90% to 99% lesion is present in the midportion of the LCX just after the takeoff of the first obtuse marginal branch. The area appears to be slightly more radiolucent than the surrounding vessel. This is an irregular plaque producing significant narrowing. FIGURE 3-11 Right coronary artery stenosis. This angiogram of the RCA is obtained in the straight LAO projection. A severe obstructive lesion is seen in the midsegment of the vessel. The segment of artery distal to the large acute marginal branch is diseased as it enters the area with the severe lesion. The distal vessel is small but relatively free of disease. FIGURE 3-12 Left anterior descending/diagonal stenosis. The image has been obtained in the AP cranial projection. In the middle of the frame, a significant stenosis of the LAD involving the bifurcation of a large diagonal branch is seen. This stenosis makes percutaneous intervention more complicated because there is a risk that flow will be compromised within this side branch. FIGURE 3-13 Total right coronary artery occlusion. A Judkins right 4.0 catheter is positioned at the ostium of the RCA. This image is obtained in the LAO view. The artery is totally occluded proximally. The lesion is said to be in the proximal portion of the vessel because it occurs before the first major acute marginal branch. The mid-RCA is defined as the portion of the artery from the end of the proximal segment to the next major acute marginal branch. The distal RCA is located from the end of the midsegment to the bifurcation of the PDA. FIGURE 3-14 In-stent restenosis of left anterior descending artery. An XB guiding catheter is present in the LMCA ostium from the radial artery approach. This image was obtained in the AP caudal projection. Before contrast injection, a stent can be visualized in the proximal portion of the LAD. A significant narrowing within the stent is consistent with in-stent restenosis. The LCX is without significant disease. However, there is a significant ostial lesion (short arrow) of the first obtuse marginal branch. FIGURE 3-15 Right coronary artery stenosis with catheter dissection. Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Computed Tomography Cardiovascular Magnetic Resonance Imaging Echocardiography Electrocardiography Cardiovascular Magnetic Resonance Imaging Positioning Occupational Lung Diseases Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Angiography Full access? Get Clinical Tree