Fig. 1.1
Gastrointestinal anthrax. (a–d) Oropharyngeal anthrax. (a) Plain CT scanning of the neck demonstrates obvious swelling of the cervical soft tissues and narrowed cavities of nasopharynx, oropharynx, and laryngopharynx. (b) Enhanced scanning demonstrates multiple enlarged lymph nodes within lesions and the neck as well as uneven enhancement. In some cases, necrosis and liquefaction can be found. (c) Inflammatory changes can be found around the lymph nodes. (d) Fluid within prevertebral space can be found, which extends from oropharynx to the superior mediastinum. (e–f) Abdominal anthrax. (e–f) Coronal CT scanning demonstrates overflow of the contrast media from active stomach and jejunum, ascites, diffusive abnormal enhancement of the gastric and intestinal mucosa, and edema of small intestines (Reprint with permission from Ozdemir H, et al. Emerg Radiol, 2010, 17(2): 161)
1.7.2.2 Abdominal Anthrax
Plain CT scanning demonstrates thickened and swollen intestinal mucosa. In some cases, intestinal obstruction and ascites may be found. However, enhanced CT scanning demonstrates leakage of contrast media into the intestinal cavity during the arterial phase (Fig. 1.1e, f).
Case Study 2
A male patient aged 43 years complained of abdominal pain, nausea, vomiting, and weakness for 2 weeks.
1.7.3 Anthrax Meningitis
CT scanning and MR imaging commonly demonstrate hemorrhagic brain parenchyma (commonly the deep gray matter or junction of gray matter and white matter), subarachnoid space, cerebral ventricles, and meninges. Enhanced scanning or imaging demonstrates diffusive abnormal enhancement of the meninges.
Case Study 3
A boy aged 12 years was hospitalized due to sudden unconsciousness and convulsion. Physical examinations found T 37 °C and P 90/min and irregular respiration and by laboratory tests, WBC 18.7 × 109/L, ESR 3 mm/h, AST 328 U/L, ALT 93 U/L, and CRP 860 mg/L (Fig. 1.2).
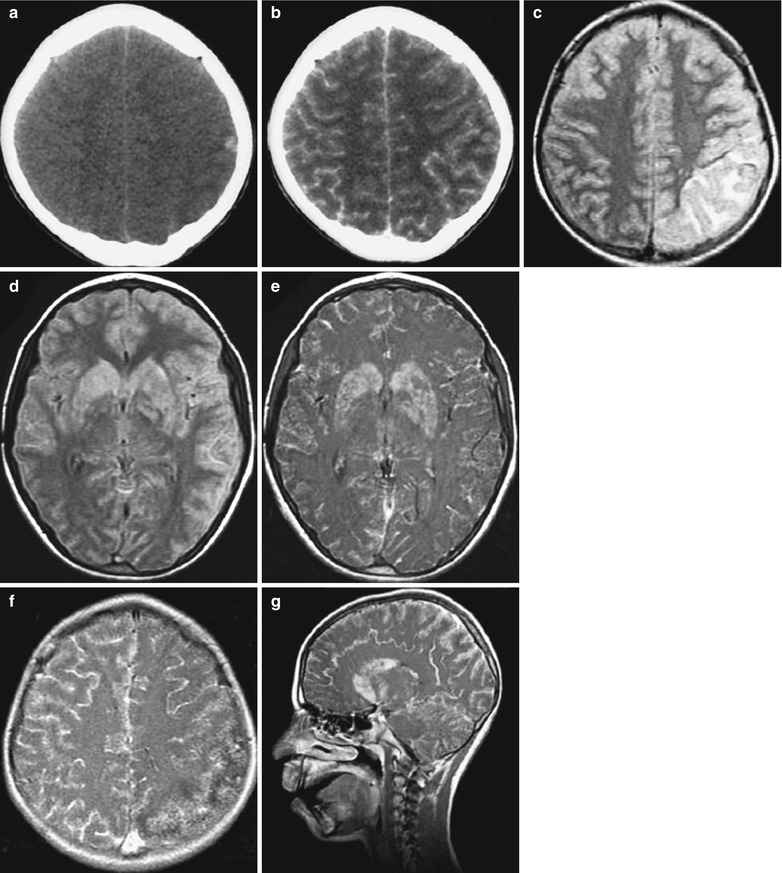
Fig. 1.2
Anthrax meningitis. (a, b) Plain CT scanning demonstrates hemorrhagic left parietal lobe and diffusive enhancement of meninges. (c, d) FLAIR imaging demonstrates high signal from the parietal lobe and basal ganglia. (e–g) Enhanced MR imaging demonstrates enhancement of the lesions in the basal ganglia and enhancement of meninges (Reprint with permission from Yildirim H, et al. Pediatr Radiol. 2006, 36(11): 1190)
1.8 Basis for Diagnosis
1.8.1 Epidemiological Data
The patients may have a history of visiting an epidemic area of anthrax in recent 2 weeks, with close contact to the diseased animals or their fur. Otherwise, the patients may have a history of eating meat from infected animals.
1.8.2 Clinical Manifestations and Diagnostic Imaging
1.8.2.1 Cutaneous Anthrax
The skin has typical changes of no purulent lesions, non-depressive painless edema, eschar, and ulceration. Based on these typical skin lesions, the diagnosis can be made.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


