2 Aortic Arch
D. Hortung, K. Hueper
2.1 Development of the Aortic Arch
During the early stages of embryonic development two pairs of aortas are present. The anterior aortas ascend from the heart, turn posteriorly within the first branchial arch, and descend as the posterior aortas. Already in embryos with 3-mm crown-heel length, the beginnings and ends of the paired aortas merge, remaining separate only in the area of the foregut. In each of the six branchial arches, connections develop between the anterior and posterior aortas, the branchial arteries. These arteries do not coexist, the first branchial arteries having already disappeared before the fifth and sixth develop. The fifth branchial artery seems to be present for a few hours only, although a few instances of its persisting have been reported.1–3 The carotid arteries develop from the cranial part of the anterior and posterior aortas. The posterior aortas give off segmental branches along their segmented body wall: 3 occipital, 7 cervical, and 12 thoracic, etc. All cervical arteries disappear, except for the sixth, which forms the subclavian artery. A longitudinal anastomosis remains on both sides to form the vertebral artery.
Thus, as a rule, the human aortic arch develops in the following way:
1.The left side of the fourth branchial artery forms part of the aortic arch, and the right side forms the beginning of the subclavian artery.
2.Parts of the posterior aortas on both sides atrophy, that is, the area between the third and fourth branchial arteries (left) and the section between the sixth segmental artery and the merged descending aorta (right).
3.The sixth branchial arteries form the beginning of the pulmonary arteries and the ductus arteriosus (Botallo’s duct). The final topographical position of the aortic arch and its branches is a product of differential growth rates of various parts of the arteries, which results in a “migration” and “merging” of branches. The main force behind these changes seems to be the optimization of hemodynamic paths combined with the descending heart.
For developmental and general aspects of the aortic arch, see the literature.4–15
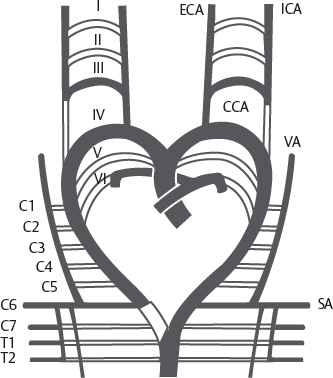
Fig. 2.1 Development of the aortic arch. I–VI, occipital segmental branches; C1–C7, cervical segmental branches; T1–T2, thoracic segmental branches; CCA, common carotid artery; ECA, external carotid artery; ICA, internal carotid artery; SA, subclavian artery; VA, vertebral artery.
2.2 “Normal” Situation (70%)
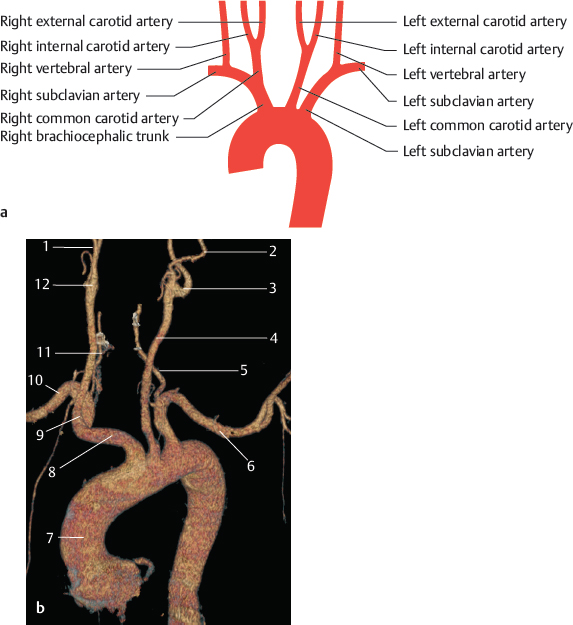
Fig. 2.2 “Normal” situation as given in textbooks (70%). Schematic (a) and MRA, VR 3D image, anterior view (b). 1 Right external carotid artery; 2 left external carotid artery; 3 left internal carotid artery; 4 left common carotid artery; 5 left vertebral artery; 6 left subclavian artery; 7 aorta; 8 right brachiocephalic trunk; 9 right common carotid artery; 10 right subclavian artery; 11 right vertebral artery; 12 right internal carotid artery.
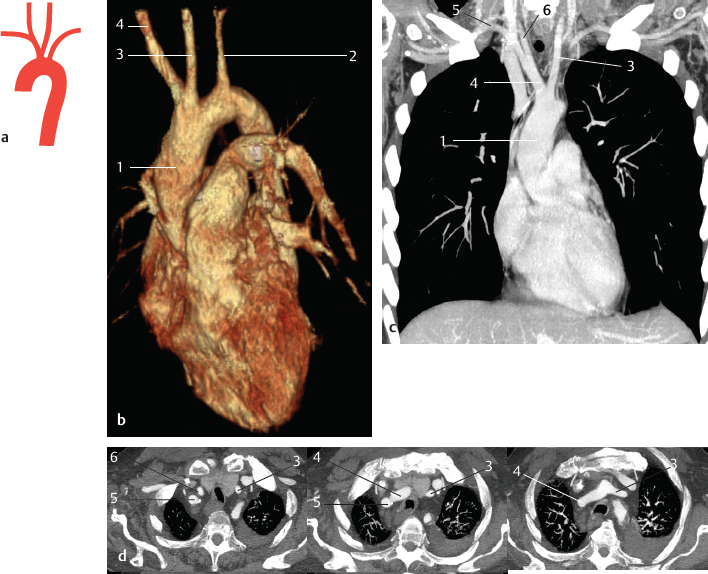
Fig. 2.3 Common origin of the right brachiocephalic trunk and left common carotid artery (~13%). Schematic (a) and contrast-enhanced CT images of two patients (b–d). Patient 1: VR 3D image, anterior view (b); MIP at the level of the common origin of the right brachiocephalic trunk and the left common carotid artery, coronal view (c). Patient 2: MIP of the supra-aortic arteries, transverse views (d). Patient with left-sided pleural effusion. 1 Aorta; 2 left subclavian artery; 3 left common carotid artery; 4 right brachiocephalic trunk; 5 right subclavian artery; 6 right common carotid artery.
2.3 Anomalies of the Trunk (23%)
The frequencies of the different types depend largely on the method of examination and racial factors (the types illustrated in Fig 2.3 and Fig 2.4 seem to be present more often in blacks than in Caucasians). Some descriptions are difficult to classify and lie between the types shown in Fig. 2.2, Fig. 2.3, and Fig 2.4. According to the literature, the types shown in Figs. 2.2–2.11 cover approximately 93% of all humans.5,8,14,16–30
Some types that are considered anomalies in humans are the rule in other mammals; for example, Fig 2.4 occurs in rodents and carnivores, Fig 2.5 in insectivores, Fig 2.6 in elephants, and Fig 2.7 in paired and unpaired ungulates.
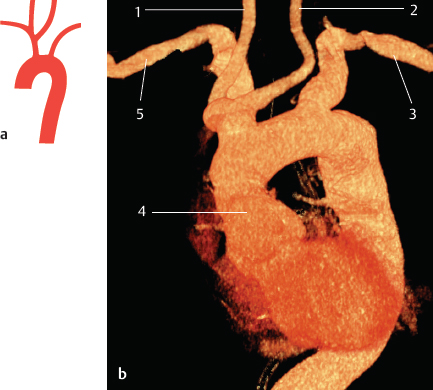
Fig. 2.4 Left common carotid artery originates from the right brachiocephalic trunk (~9%). Schematic (a) and contrast-enhanced CT of the thoracic aorta, VR 3D image, anterior view (b). 1 Right common carotid artery; 2 left common carotid artery; 3 left subclavian artery; 4 aorta; 5 right subclavian artery.
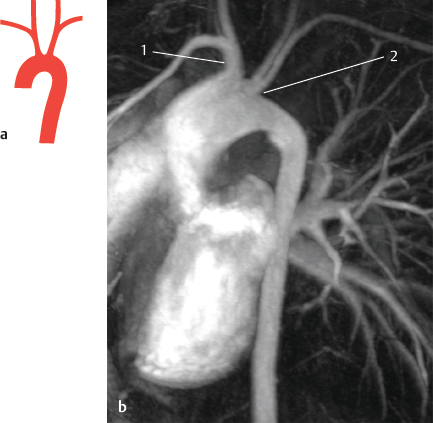
Fig. 2.5 Right and left brachiocephalic trunk (<1%). Schematic (a) and MRA, VR 3D image, sagittal oblique view (b). 1 Right brachiocephalic trunk; 2 left brachiocephalic trunk.

Fig. 2.6 Trunk formation of both carotid arteries (bicarotid) (<0.1%). Schematic.
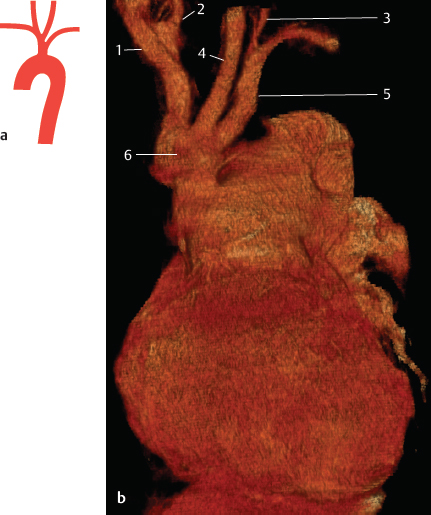
Fig. 2.7 Common brachiocephalic trunk (<0.1%). Schematic (a) and contrast-enhanced CT of the thoracic aorta, VR 3D image, anterior view (b). The CT image shows the common brachiocephalic trunk in a 24-year-old woman with a truncus arteriosus as a congenital cardiac anomaly. 1 Right subclavian artery; 2 right common carotid artery; 3 left vertebral artery; 4 left common carotid artery; 5 left subclavian artery; 6 common brachiocephalic trunk.

Fig. 2.8 Right subclavian artery originates from a bicarotid trunk (<0.1%). Schematic.

Fig. 2.9 Left subclavian artery originates from a bicarotid trunk (<0.1%). Schematic.

Fig. 2.10 Only a left brachiocephalic trunk (<0.1%). Schematic.

Fig. 2.11 No brachiocephalic trunk (<0.1%). Schematic.
2.4 Vertebral Artery as a Direct Branch of the Aortic Arch (4%)
When a segmental artery persists more cranial than the sixth cervical artery, the left vertebral artery will branch from the aortic arch. In such cases, the vertebral artery enters the vertebral column through a more cranial transverse foramen. The vertebral artery can have two origins when the longitudinal anastomosis to the sixth segmental artery remains open. In extremely rare instances, the right vertebral artery originates from the aortic arch. In such cases, either all the beginning part of the right fourth branchial artery forms the aortic arch or there is a variety of the type shown in Section 2.6 with a subsequent “migration” of the origin of the artery.31–33
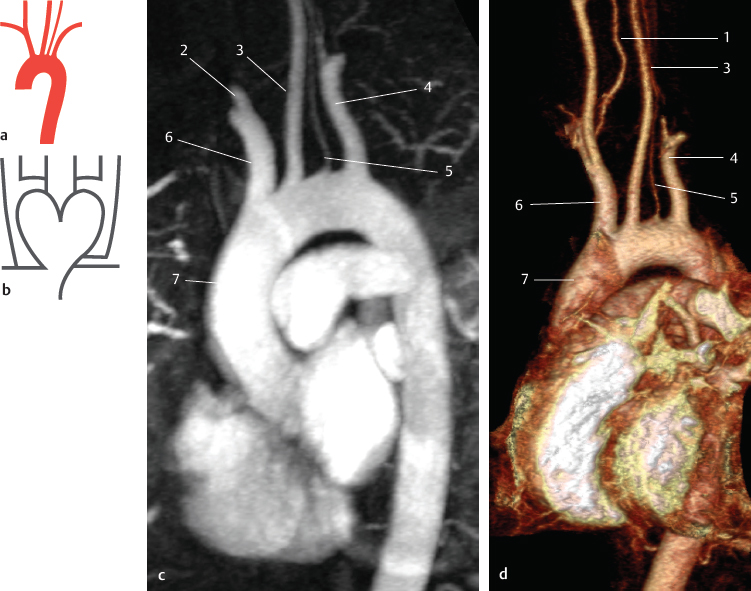
Fig. 2.12 Left vertebral artery as the penultimate branch of the aortic arch (3%). Schematics of the arterial variation (a), its development (b), and MRA images of the arterial variation (c,d), both of the same patient. MIP of the thoracic aorta and the supra-aortic vessels in an oblique sagittal view (c), VR 3D image in an oblique sagittal view (d). 1 Right vertebral artery; 2 right common carotid artery; 3 left common carotid artery; 4 left subclavian artery; 5 left vertebral artery; 6 right brachiocephalic trunk; 7 aorta.

Fig. 2.13 Left vertebral artery as the penultimate branch of the aortic arch; left common carotid artery originating from the brachiocephalic trunk (<1%). Schematic.

Fig. 2.14 Left vertebral artery as the last branch of the aortic arch (<1%). Schematic.

Fig. 2.15 Left vertebral artery as the last branch of the aortic arch; left common carotid artery originating from the brachiocephalic trunk (<0.1%). Schematic.

Fig. 2.16 Left vertebral artery as the last branch of the aortic arch; a common brachiocephalic trunk (<0.1%). Schematic.
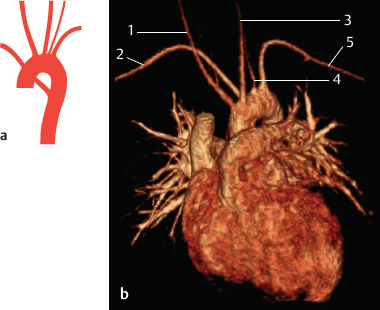
Fig. 2.17 Vertebral artery branches before the left subclavian artery, but the last branch of the aortic arch is the right subclavian artery (<0.1%). Schematic (a) and MRA, VR 3D image, anterior view (b). 1 Right common carotid artery; 2 right subclavian artery; 3 left common carotid artery; 4 left vertebral artery; 5 left subclavian artery.
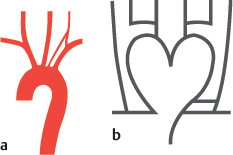
Fig. 2.18 Two roots of the vertebral artery, one penultimate branch of the aortic arch (<1%). Schematics of the arterial variation (a) and its development (b).

Fig. 2.19 Both vertebral arteries directly branch from the aortic arch (<0.1%). Schematic.
2.5 Arteria Thyroidea Ima as a Direct Branch of the Aortic Arch (1%)
The overall frequency of the lowest thyroid artery (arteria thyroidea ima) is approximately 6%: it arises from the brachiocephalic trunk in 3% of all cases; from the right common carotid artery in 1%; from the aortic arch in 1%; and less frequently from the internal thoracic artery, subclavian artery, and inferior thyroid scapular artery. Two arteria thyroidea ima have also been described. This artery is of importance in surgeries performed caudal to the isthmus of the thyroid gland. For general features, see the literature.8,9,34–40
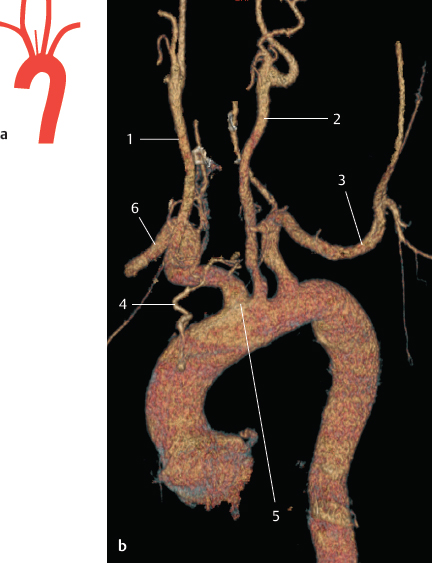
Fig. 2.20 Arteria thyroidea ima as a direct branch of the aortic arch (1%). Schematic (a) and contrast-enhanced CT, VR 3D image, anterior view (b). 1 Right common carotid artery; 2 left common carotid artery; 3 left subclavian artery; 4 arteria thyroidea ima; 5 right brachiocephalic trunk; 6 right subclavian artery.
2.6 Right Subclavian Artery as the Last Branch of the Aortic Arch (Arteria Lusoria) (1%)
In this situation, the right subclavian artery always turns to the right behind the other branches. It is located behind the esophagus in 80% of all cases, between the esophagus and trachea in 15%, and in front of the trachea or the main bronchi in 5%. This position results in dysphagia or dyspnea.8,35,40–44 In most cases, the right recurrent laryngeal nerve is absent, but there are direct branches to the trachea and esophagus from the vagus. If the right vertebral artery branches from the right common carotid artery (see Fig. 2.24a), a nerve, comparable to the recurrent laryngeal nerve, winds around the artery.
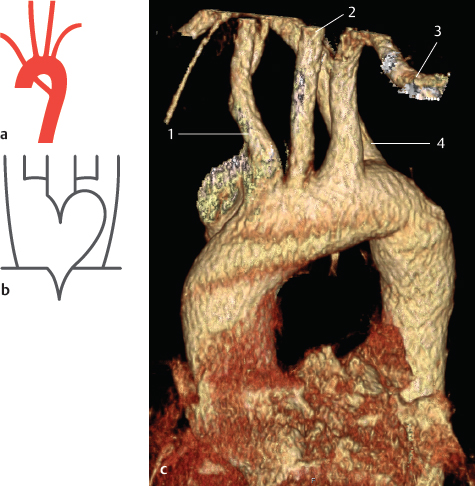
Fig. 2.21 Right subclavian artery as the last branch of the aortic arch, other arteries originate normally (<1%). Schematics of the arterial variation (a), its development (b), and contrast-enhanced CT of the arterial variation (c), VR 3D image, anterior view. The scan field of view in c is limited to the thorax, so that the supra-aortic vessels are not displayed in their entire course. 1 Right brachiocephalic trunk; 2 left common carotid artery; 3 left subclavian artery; 4 right subclavian artery.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


