Etiology
Mucoceles of the appendix are caused by excessive mucous production secondary to retention cyst (simple) (18%), mucosal hyperplasia (20%), mucinous cystadenoma (52% to 84%), or mucinous cystadenocarcinoma (10% to 20%). They occur in males twice as frequently as females and most often in the fifth or sixth decade. The incidence of mucocele of the appendix is 0.2% and 0.3% of all appendectomies.
Ultrasound Findings
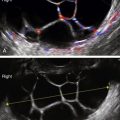
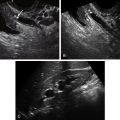
Mucocele of the appendix is an elongated tubular mass with a very specific onion-skin texture of the internal structure, giving the appearance of echogenic layers. There is no internal blood flow, and Doppler signal is confined to the outer walls of the mass. Although the mass is usually seen using transvaginal ultrasound, it is also usually visible using a transabdominal approach in the right lower quadrant. The dreaded complication of mucocele rupture or leak is pseudomyxoma peritonei, which appears as diffuse gelatinous ascites.
Differential Diagnosis
Most cases are incidental findings and often misdiagnosed. In women, it is commonly diagnosed as an ovarian or tubal mass. The correct preoperative diagnosis based on imaging studies is made in only 15% to 29% of cases.
The appendix is typically located in the right lower quadrant just cephalad to the right adnexa; therefore it is important to consider an appendiceal etiology for a right lower quadrant tubular mass with or without pelvic pain. Diagnostic possibilities for a complex, right lower quadrant mass include an ovarian etiology, although the tubular appearance of an appendiceal mucocele is more easily confused with a tubal lesion such as a hydrosalpinx, tubo-ovarian abscess, or endometriosis. It is essential to identify the uterus and ovaries separately from the mass to identify a bowel etiology. Once the origin of the mass is suspected to be appendix, the differential diagnosis includes acute inflammation of the appendix (appendicitis), malignancy (adenocarcinoma), mucocele, carcinoid, and appendiceal endometriosis. Other diagnostic possibilities include a colonic mass or mesenteric cyst. The sonographic appearance of the mucocele is very characteristic, even pathognomonic, with the onion-skin texture and nonvascular center of a tubular mass. Other etiologies for an appendiceal mass are almost impossible to distinguish from one another without a history such as acute pain and fever, or endometriosis.
See Bowel Diseases.
Clinical Aspects and Recommendations
Appendiceal mucoceles are symptomatic in about half of cases. The most common symptoms are a palpable mass and abdominal pain. The treatment is appendectomy to prevent rupture and to diagnose any malignant component. If the mucocele is the result of a cystadenocarcinoma and the tumor has spread, more extensive surgery is needed.
The feared complication of this entity is pseudomyxoma peritonei, which results from the dissemination of the mucinous cells because of rupture of the mucocele. This complication is very serious and extremely hard to treat; it can lead to intestinal obstruction and death. Treatment typically involves a combination of surgery for debulking and intraperitoneal chemotherapy. Although the prognosis for appendiceal mucocele without complication is excellent, the 3-year survival of patients with pseudomyxoma peritonei is reportedly 81%.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


