Arm and Elbow Joint
Anatomy and Techniques
Arm Anatomy
Position 1: Anterior Compartment Proximal
The neurovascular bundle on the medial aspect of the arm provides a useful landmark to begin to view the anatomy of the proximal arm. The bundle comprises the brachial artery and veins, with the median nerve anteriorly and ulnar nerve posteriorly (Fig. 5.1). A number of smaller cutaneous nerves are all found here. The medial antebrachial nerve lies superficial and anterior while the medial brachial cutaneous nerve lies superficial and posterior. At a very high level, the radial nerve is also noted in this compartment, posterior to the brachial artery. It will soon pass into the posterior compartment as it traverses from medial to lateral posterior to the humerus. The coracobrachialis muscle is anterolateral to the bundle. High in the anterior compartment, well above the deltoid insertion, the pectoralis muscle and tendon is found as it passes to its insertion on the humerus. Deep to this are the two heads of biceps which overlie the coracobrachialis muscle (Fig. 5.2). The other important nerve structure is the musculocutaneous nerve which passes through the coracobrachialis in its posterior portion to come to lie between this muscle and the overlying biceps.
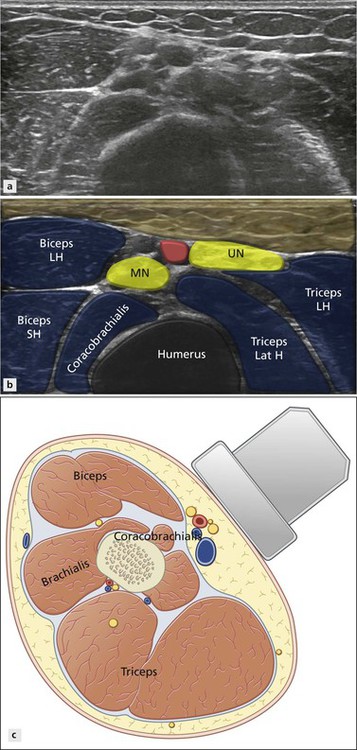
Figure 5.1 Axial medial upper arm. The brachial artery and surrounding nerves are a useful landmark.
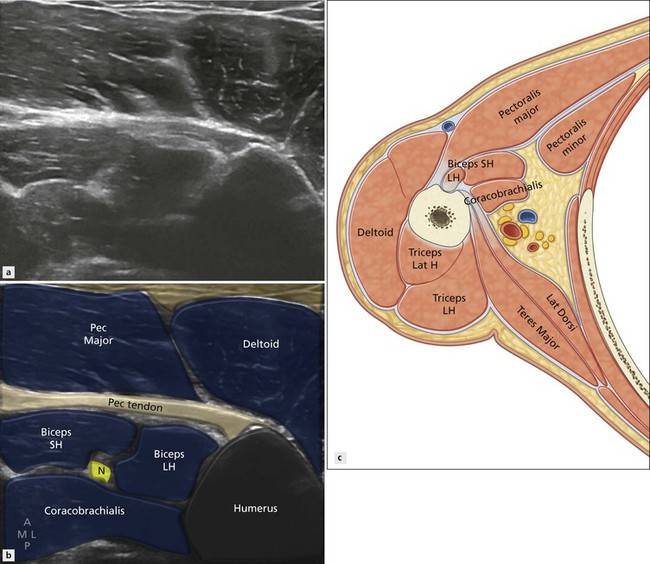
Figure 5.2 Axial medial upper arm. The triceps insertion is a marker for the two heads of biceps coming together with the musculocutaneous nerve (N) posteriorly.
Position 2: Anterior Compartment Distal
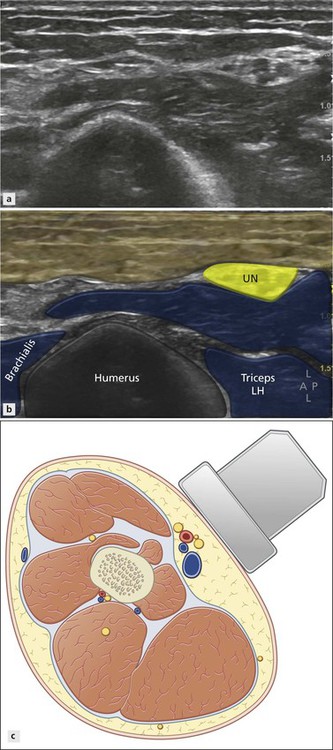
As the probe is passed a little more distally, the brachialis muscle that has an origin from the anteriolateral aspect of the humerus appears (Fig. 5.3). As this muscle grows distally, the coracobrachialis diminishes towards its insertion medially. Below the insertion of the coracobrachialis, the biceps and brachialis muscles dominate the anterior compartment (Fig. 5.4). At this level, the ulnar nerve has moved a little more posteriorly and is now often contained in a little pouch on the medial surface of the medial head of triceps (Fig. 5.5). The median nerve maintains its relationship with the brachial artery. The musculocutaneous nerve emerges from coracobrachialis to lie between the biceps muscle anteriorly and the brachialis muscle posteriorly as it moves laterally.
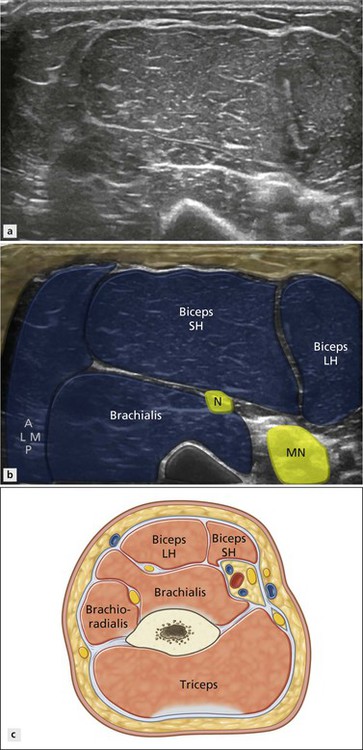
Figure 5.3 Axial anterior arm. The biceps and brachialis muscles dominate the anterior compartment. The musculocutaneous nerve (N) lies between them.
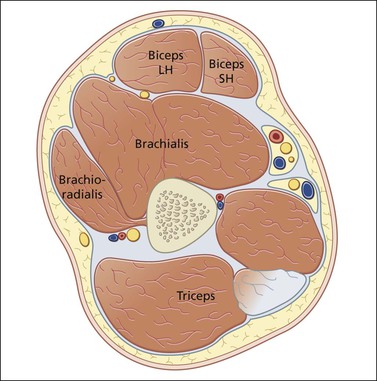
Figure 5.4 The ulnar nerve has separated from the brachial artery and passes to a compartment adjacent to the medial head of triceps. The radial nerve has passed to the lateral aspect of the humerus.
Position 3: Posterior Compartment Proximal
The posterior compartment contains the three heads of triceps and deltoid. In the proximal arm, however, the medial head has yet to appear. The long head arises from the infraglenoid tubercle of the scapula. It forms the central third of the bulk of the extensor compartment. The lateral head also arises from the dorsal surface of the humerus. Proximally, the lateral relation of the triceps is the deltoid muscle, straddling both anterior and posterior compartments. The medial relation is the tendon of latissimus dorsi. The radial nerve passes below teres major and enters its groove on the posterior aspect of the humerus.
Position 4: Posterior Compartment Distal
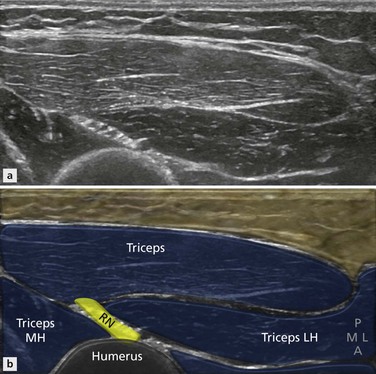
The medial head of triceps has a much lower origin than the lateral or long head. It arises below the insertion of teres major, and just below the groove for the radial nerve. In the proximal arm, therefore, prior to the radial nerve passing posterior to the humerus, the muscle posterior to it is the long head, not the medial head. As the radial nerve emerges lateral to the humerus, all three muscles of the posterior compartment are present and visible (Fig. 5.6). The radial nerve now lies lateral between the anterior and posterior compartments, that is, between the brachialis muscle anteriorly and the lateral head of triceps posteriorly, along with the posterior antebrachial cutaneous nerve.
As the radial nerve is followed distally, it passes around the lateral border of brachialis. As it does this, it gains two new lateral relations: the brachioradialis (Fig. 5.7) first, then extensor carpi radialis longus as it gradually moves towards the anterior compartment. These two muscles of the forearm compartment are covered more fully in Chapter 10.
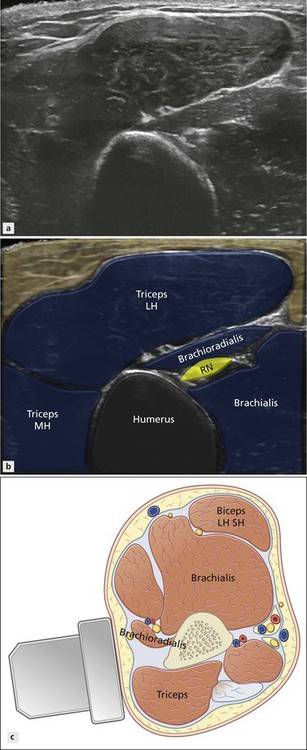
Figure 5.7 Axial anterolateral lower arm. The radial nerve moves between the brachioradialis and brachialis before it enters the anterior elbow.
Elbow Anatomy and Techniques
Position Variations
For children with elbow joint effusions, an option is to have the child sit on the parent’s lap, facing them with one knee on either side of the parent. The parent can cuddle the child whilst making the posterior aspect of the elbow available for ultrasound examination and aspiration.