Arthritis and Other Abnormalities of the Metatarsophalangeal and Interphalangeal Joints
Anatomic Considerations
The metatarsophalangeal joints of the toes are condyloid joints characterized by the articulation of the rounded articular surfaces of the metatarsal heads into the shallow concavities of the articular surfaces of the proximal end of the first phalanges (Fig. 18.1). Each joint is lined with synovium and the ample synovial space allows for intra-articular placement of needles for injection and aspiration. The metatarsophalangeal joints have a dense joint capsule and strong plantar and collateral ligaments, although fracture and subluxation may still occur (Figs. 18.2 and 18.3). The metatarsophalangeal joints of the toes are also susceptible to overuse and misuse injuries with resultant inflammation and arthritis. The interphalangeal joints of the toes are ginglymoid hinge joints which have extensive flexion and more limited extension due to the limitation of the metatarsal and collateral ligaments (Figs. 18.2 and 18.4).
 FIGURE 18.1 Anatomy of the metatarsophalangeal joints. (From Weber J, Kelley J. Health Assessment in Nursing. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
Clinical Correlates
The metatarsophalangeal joints of the toes are synovium lined condyloid joints characterized by the articulation of the rounded articular surfaces of the metatarsal heads into the shallow concavities of the articular surfaces of the proximal end of the first phalanges (Fig. 18.4). The primary function of the metatarsophalangeal and interphalangeal joints of the toes is to aid in the gripping function of the foot. The articular cartilage of the metatarsophalangeal and interphalangeal joints of the toes are susceptible to damage, which left untreated, will result in arthritis with its associated pain and functional disability. Osteoarthritis is seen in the metatarsophalangeal and interphalangeal joints of the toes which results in pain and functional disability, with rheumatoid arthritis, posttraumatic arthritis, and crystal arthropathy also causing arthritis of the metatarsophalangeal and interphalangeal joints of the toes. Gout selectively afflicts the metatarsophalangeal joint of the first toe and is called podagra (Figs. 18.5 and 18.6). Less common causes of arthritis-induced pain of the metatarsophalangeal and interphalangeal joints of the toes include other collagen vascular diseases, infection, psoriatic arthritis, villonodular synovitis, and Lyme disease (Figs. 18.7 and 18.8). Acute infectious arthritis of the metatarsophalangeal joints of the toes is best treated with early diagnosis, with culture and sensitivity of the synovial fluid, and prompt initiation of antibiotic therapy. The collagen vascular diseases generally manifest as a polyarthropathy rather than a monoarthropathy limited to the metatarsophalangeal and interphalangeal joints of the toes, although pain of the metatarsophalangeal and interphalangeal joints of the toes, secondary to the collagen vascular diseases, responds exceedingly well to ultrasound-guided intra-articular injection.
Patients with pain of the metatarsophalangeal and interphalangeal joints of the toes secondary to arthritis, gout, synovitis,
and collagen vascular disease–related joint pain, complain of pain that is localized to the head of the metatarsals. Activity, including walking and weight bearing makes the pain worse, with rest and heat providing some relief. The pain is constant and characterized as aching in nature. Sleep disturbance is common with awakening when patients roll over onto the affected foot. Some patients complain of a grating, catching, or popping sensation with a range of motion of the joints, and crepitus may be appreciated on physical examination.
and collagen vascular disease–related joint pain, complain of pain that is localized to the head of the metatarsals. Activity, including walking and weight bearing makes the pain worse, with rest and heat providing some relief. The pain is constant and characterized as aching in nature. Sleep disturbance is common with awakening when patients roll over onto the affected foot. Some patients complain of a grating, catching, or popping sensation with a range of motion of the joints, and crepitus may be appreciated on physical examination.
 FIGURE 18.2 A, B: Cutaneous nerves of the sole of the foot. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:154.) |
 FIGURE 18.3 Plain radiograph of metatarsophalangeal joint showing a complete dislocation. (From Bucholz RW, Heckman JD. Rockwood & Green’s Fractures in Adults. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.) |
Functional disability often accompanies the pain associated with the many pathologic conditions that affect the metatarsophalangeal joints of the toes. Patients will often notice increasing difficulty in performing their activities of daily living and tasks that require standing, walking, or weight bearing. If the pathologic process responsible for pain of metatarsophalangeal and interphalangeal joints of the toes is not adequately treated, the patient’s functional disability may worsen and muscle wasting and ultimately frozen metatarsophalangeal and interphalangeal joints of the toes may occur.
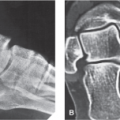
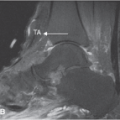
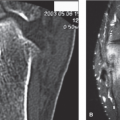
Plain radiographs are indicated in all patients who present with pain of the metatarsophalangeal and interphalangeal joints of the toes (Fig. 18.9). Based on the patient’s clinical presentation, additional testing may be indicated including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI or ultrasound of the metatarsophalangeal and interphalangeal joints of the toes is indicated if fracture, effusion, tendinopathy, crystal arthropathy, joint mice, synovitis, foreign body, bursitis, or ligamentous injury is suspected (Figs. 18.10 to 18.13).
Ultrasound Technique
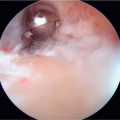
To perform ultrasound evaluation of the metatarsophalangeal and interphalangeal joints of the toes, the patient is placed in the supine position with the knee flexed so that the plantar surface of the affected foot rests comfortably on the examination table. With the patient in the above position, the dorsal surface of the metatarsophalangeal joint of the affected toe is identified by palpation. A high-frequency small linear ultrasound transducer is placed in a longitudinal position over the metatarsophalangeal joint of the affected toe and an ultrasound survey scan is taken (Figs. 18.14 and 18.15). The hypoechic metatarsophalangeal joint space is identified between the head of the metatarsal and the base of the proximal phalanges. When the joint space is identified, the joint is evaluated for the presence of arthritis, synovitis, effusion, crystal deposition, and abnormal masses including ganglion cysts (Figs. 18.16 to 18.25). Ultrasound and color Doppler are used to identify synovitis and areas of neovascularity in healing tendons and joints (Figs. 18.26 to 18.30). After the metatarsophalangeal joints and surrounding structures are evaluated the transducer is slowly moved distally to evaluate each interphalangeal joint of the toes (Figs. 18.31 and 18.32).
Related posts:
 Arthritis and Other Abnormalities of the Subtalar Joint
Arthritis and Other Abnormalities of the Subtalar Joint
 Arthritis and Other Abnormalities of the Ankle Joint
Arthritis and Other Abnormalities of the Ankle Joint
 Anterior Tarsal Tunnel Syndrome and Other Abnormalities of the Deep Peroneal Nerve
Anterior Tarsal Tunnel Syndrome and Other Abnormalities of the Deep Peroneal Nerve
 Retrocalcaneal and Achilles Bursitis
Retrocalcaneal and Achilles Bursitis
 Calcaneal Spurs
Calcaneal Spurs
 Plantar Fasciitis and Other Abnormalities of the Plantar Fascia
Plantar Fasciitis and Other Abnormalities of the Plantar Fascia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


