Fig. 17.1
A small superficial abscess (arrow) in the gluteal subcutaneous tissues that was not detectable by transanal ultrasound but imaged using transperineal ultrasound
To overcome the poor visualization of fistulous tracts, clarify the course of patent tracts, and correctly classify perianal fistulas, hydrogen peroxide transanal ultrasound is frequently used [1–3]. However, this procedure does not avoid the risks of misinterpretation. In fact, after the injection of hydrogen peroxide into the external opening, gas within the tract may produce shadowing that mimics extensions. This phenomenon can occur with any tract that contains air, leading, for example, to intersphincteric fistulas being inadvertently classified as transsphincteric (Fig. 17.2). Similarly, when the external opening is close to the anal opening and it is difficult to detect the presence of severe perianal disease, indurations, and skin tags, hydrogen peroxide may leak from the external opening across the skin and reflux into the anal canal and the rectum, thus hampering sonographic visualization in addition to mimicking at transperianal examination the presence of an intasphincteric or complex fistula. In fact, air in the anal canal, in particular in patients with anal ulcers, has an appearance similar to that of hydrogen peroxide and results in brightly echogenic shadowing that seems to arise from the lumen of the anal canal, suggesting a patent tract communicating with the anal lumen. Likewise, setons, surgical sutures, and hemorrhoidal bands in the anal wall should be identified before hydrogen peroxide injection, because these are echogenic and may simulate gas within a fistula or small intramural abscesses (Fig. 17.3).

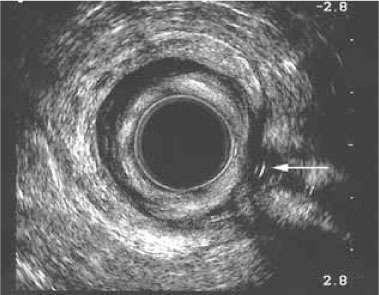
Fig. 17.2
Transverse transanal sonogram at the upper anal canal level, showing intersphincteric horseshoe extension (arrows). Gas in the fistula causes acoustic shadowing, which could be mistaken for a transsphincteric tract
Fig. 17.3
Transanal sonogram at the level of the upper anal canal, showing a seton within the fistula (arrow)
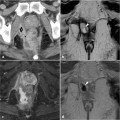
An exact ultrasonographic definition and classification of complex perianal fistulas and perianal abscesses may be limited using bi-dimensional evaluation. Transanal ultrasound and transperineal ultrasound are disadvantaged by their inability to image the coronal and transversal planes, respectively. Therefore, using conventional transanal ultrasound it is difficult to distinguish supra- from infralevator extensions and abscesses (Fig 17.4




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
