Fig. 28.1
A 46-year-old male patient with Crohn’s disease. There is a very subtle posterior linear tract on the T2-weighted axial image (a), with linear enhancement after intravenous gadolinium as seen on the axial contrast-enhanced fat-saturated T1-weighted image (b). This active simple intersphincteric fistula was initially detected by means of transperineal ultrasound

Fig. 28.2
A female patient with previously diagnosed Crohn’s disease. On axial (a) and sagittal (b) T2-weighted images and on axial contrast-enhanced fat-saturated (c) and sagittal (d) T1- weighted images, there is midline obliteration of the normal, thin fat layer of the anovaginal septum by intermediate T2 signal intensity tissue with moderate enhancement. Correlation with symptoms and transperineal ultrasound allowed the diagnosis of a collapsed anovaginal fistula
A not infrequent source of interpretation error for the inexperienced radiologist involves the presence of veins running in the ischioanal spaces, which is not unusual but can they be misinterpreted as fistulas. Correct identification of these normal, enhancing structures should rely on their thin-walled, tortuous, and branching appearance, and on their usual symmetric presence on both sides (Fig. 28.3) [3].
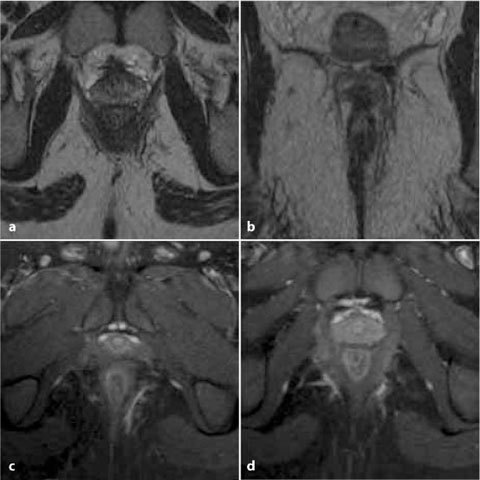
Fig. 28.3
Veins running symmetrically in the ischioanal fat spaces, seen as thin, linear structures with branching on axial (a) and coronal (b) T2-weighted images, enhancing after intravenous gadolinium administration on axial post-contrast fat-saturated (c, d) T1-weighted images. These findings did not correspond to clinical or transperineal ultrasound evidence of perianal inflammation and should not be mistaken for fistulas
Sometimes, the classification of perianal inflammatory disease on MRI studies according to the Parks’ and St. James’ University Hospital (SJUH) schemes may prove challenging for the radiologist, with a non-negligible interpretation uncertainty. Not unexpectedly, interobserver agreement has been reported to be significantly higher for the detection of abscesses and horseshoe fistulas than for simple tracts [1, 4]. In our experience, the MRI-based SJUH staging system is more easily adopted in everyday radiologic practice and we strongly suggest its application in reporting MRI examinations.
A fistulous external opening is not an issue at MRI, since its presence and draining status are always assessed clinically and are generally evident at surgical inspection. According to Goodsall’s rule, a fistula having an external orifice situated behind the transverse anal line opens into the anal canal in the midline posteriorly [2].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


