Abstract
Atelectasis is loss of lung volume and a very common observation, with an appearance on the chest x-ray that is often nonspecific, but shift of normal structures may confirm the diagnosis. Atelectasis in an intensive care patient is usually the result of retained bronchial secretions and mucous plugs, but lobar atelectasis in the outpatient is most likely the result of an endobronchial tumor.
Keywords
airway obstruction, carcinoid, compressive atelectasis, lung cancer, lymphoma, metastases, mucous plugs, resorption atelectasis, tuberculosis
Questions
- 1.
Which of the following abnormalities are present on the posteroanterior (PA) chest radiograph in Fig. 13.1 ?
- a.
Right upper lobe opacification.
- b.
Juxtaphrenic peak.
- c.
Displacement of the horizontal fissure.
- d.
Deviation of the trachea.
- e.
All of the above.

Fig. 13.1
- a.
- 2.
Which one of the following is most likely to cause atelectasis?
- a.
Metastasis.
- b.
Adenocarcinoma.
- c.
Lymphoma.
- d.
Squamous cell carcinoma.
- e.
Sarcoidosis.
- a.
- 3.
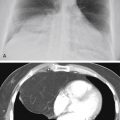
The case illustrated in Fig. 13.2 is an example of which of the following types of atelectasis?
- a.
Compressive.
- b.
Obstructive.
- c.
Cicatrizing.
- d.
Relaxation.
- e.
Adhesive.

Fig. 13.2
- a.
Match the following types of atelectasis with the disease entities listed in the right column:
|
|
|
|
|
|
|
|
|
|
Discussion
Atelectasis is loss of lung volume 221 that may involve all or parts of the lung. Chest radiographic findings of atelectasis include the following: (1) increased opacity; (2) crowding and reorientation of pulmonary vessels 445 ; (3) displacement of fissures 253 ; (4) elevation of the diaphragm; (5) displacement of the hilum; (6) crowding of ribs; (7) compensatory overinflation of the normal lung; (8) shift of the mediastinum; (9) cardiac rotation 287 ; (10) bronchial rearrangement 627 ; and (11) juxtaphrenic peak ( Fig. 13.3 ). 112 On occasion, the change in position of an abnormal structure, such as a calcified granuloma, may also provide additional clues to the diagnosis. 481 As with other pulmonary problems, the radiologic signs of atelectasis are variable, ranging from nonspecific signs such as increased opacity to specific signs such as displacement of the fissures and a shift of the mediastinum. 287 Perhaps the most specific sign is displacement of the fissures, indicating a loss of volume in a specific lobe. 656 , 657
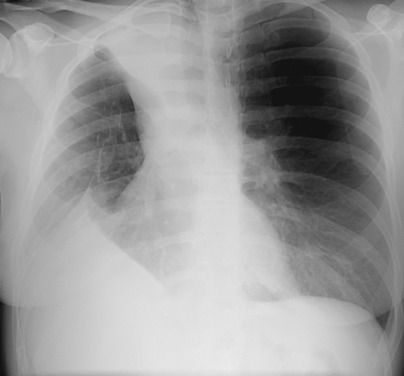
Right upper lobe atelectasis (see Fig. 13.1 ) is usually recognized by observation of findings that include right upper lobe opacity with elevation of the horizontal fissure. The horizontal fissure may even appear to be bowed or rotated upward and medially. The mediastinum may shift toward the opacity with deviation of the trachea. Elevation of the right hemidiaphragm and a juxtaphrenic peak are frequently observed additional findings of right upper lobe atelectasis. The juxtaphrenic peak is a triangular opacity extending upward from the diaphragm. It may be caused by traction on either an inferior accessory fissure or the inferior pulmonary ligament 221 (answer to question 1 is e ). The lateral view shows upper anterior opacity with upward shift of the horizontal fissure, anterior shift of the oblique fissure, and compensatory overinflation of the middle and lower lobes.
Right middle lobe atelectasis causes a combination of increased opacity that silhouettes the right heart border 349 with inferior displacement of the horizontal fissure. The lateral view often shows anterior shift of the lower portion of the oblique fissure ( Fig. 13.4, A and B ). Right middle lobe atelectasis is most often caused by bronchial obstruction (see Fig. 13.4, C ).

Right lower lobe atelectasis causes increased opacity in the lower thorax without silhouetting of the right heart border. There is inferior and medial shift of the oblique fissure. Remember, the oblique fissure is not normally seen on the PA view, 230 but the shift that results from right lower lobe atelectasis often causes the fissure to become visible on the PA view ( Fig. 13.5 ).

Left upper lobe atelectasis causes a poorly defined left perihilar opacity that appears to be separated from the mediastinal border by a hyperlucency or air crescent (the Luftsichel sign) that highlights the aortic arch. 45 Compensatory overaeration of the superior segment of the left lower lobe accounts for the hyperlucency that is interposed between the mediastinum and opaque upper lobe ( Fig. 13.6, A-C ). Left upper lobe atelectasis assumes a very characteristic appearance on the lateral view with an anterior opacity that is sharply defined posteriorly by the oblique fissure, which is displaced anteriorly (see Fig. 13.6, B ). Because of compensatory overinflation of the right upper lobe, which may give the appearance of herniating across the midline, the opacity of left upper lobe atelectasis does not obliterate the retrosternal clear space.

Left lower lobe atelectasis causes a triangular opacity behind the heart ( Fig. 13.7 ). The lateral border is sharp because of the inferior medial shift of the oblique fissure. This often produces the appearance of a line that parallels the heart border. The lateral view confirms a poorly defined opacity that projects over the lower vertebral bodies and silhouettes the left leaf of the diaphragm.

Complete opacification of a hemithorax with a shift of the mediastinum toward the opacity is classic for atelectasis ( Fig. 13.8 ). In these cases, the shift of the mediastinum toward the opaque side confirms the atelectasis, but the opacification obscures the lung and any underlying abnormalities. The diagnostic signs of complete atelectasis of the right lung are not significantly different from those of complete atelectasis of the left lung. In contrast with atelectasis, the completely opaque hemithorax with shift of the mediastinum away from the opacity is most often due to a large pleural effusion.

Because the right lung has three lobes, combinations of atelectasis of two lobes may cause some unique radiologic appearances. 330 Right upper and right middle lobe atelectasis causes a large opacity involving the right upper thorax, obscuring the right upper lobe vessels and silhouetting the heart border, and the diaphragm is elevated with the appearance of a juxtaphrenic peak. 112 The lateral view holds the key to the correct diagnosis ( Fig. 13.9, A and B ). The entire oblique fissure is shifted anteriorly to resemble the left oblique fissure position in left upper lobe atelectasis. The horizontal fissure is not visualized when it is surrounded by an atelectatic lung. In contrast, right middle and right lower lobe atelectasis cause an inferior shift of both the horizontal fissure and posterior portion of the oblique fissure. Compensatory overinflation of the upper lobe displaces the fissures inferiorly and produces a sharp interface with the collapsed lobes that may appear to parallel the diaphragm and thus mimic elevation of the diaphragm or even a subpulmonic effusion. When the opacity silhouettes the pulmonary vessels, atelectasis of the middle and lower lobes should be suspected ( Fig. 13.10, A and B ).

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


