Clinical Presentation
The patient is a 59-year-old disabled man with longstanding left hemiparesis after intracerebral hemorrhage secondary to right basal ganglia atrioventricular (AV) malformation. Patient now presents with chronic headaches and torticollis. The patient’s head and neck are rigid on physical examination.
Imaging Presentation
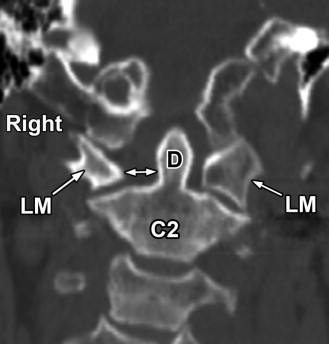
Stable appearance of the brain is compared with multiple previous magnetic resonance (MR) studies. On cervical spine radiographs, the head is tilted down and rotated to the left ( Fig. 12-1 ) consistent with torticollis. On computed tomography (CT) scan of the cervical spine, there is clockwise rotatory subluxation of the C1 vertebra relative to C2 ( Figs. 12-2 to 12-5 ) .




Discussion
Atlantoaxial rotatory fixation (AARF) is also called atlantoaxial rotatory subluxation or fixed atlantoaxial rotatory subluxation . In AARF, the atlas (C1) is either rotated about the odontoid process or the C1 lateral mass on one side is anteriorly subluxed and rotated relative to the relatively fixed C1-2 facets on the opposite side. The degree of atlantoaxial “rotation” in most cases occurs within the normal range of rotation of the atlantoaxial joint.
AARF is one cause of acquired torticollis and is more commonly encountered in children than in adults) . Although considered by some to be rare in adults, the radiographic appearance of AARF is not uncommonly seen in adults in routine practice. AARF may occur spontaneously, secondary to spasmodic torticollis, often after an upper respiratory infection, after major or minor cervical trauma, secondary to C1-2 arthritis (osteoarthritis, rheumatoid arthritis, and ankylosing spondylitis), or congenital anomalies, or is associated with infection (Grisel’s syndrome). Atlanto-occipital subluxation commonly occurs in patients with Down syndrome. Mongolism may also be associated with atlanto-occipital subluxation (AOS) and AARF. Atlantoaxial rotary fixation has been reported after disabling cerebral infarction, caused by constant head posturing to the same side (see Figs. 12-1 to 12-5 ).
AARF may be mistakenly diagnosed on radiographic images in normal children. Relatively minor degrees of apparent AARF or nonfixated C1-2 rotary subluxation in children may be considered within normal limits. In the absence of trauma or torticollis, this diagnosis should always be questioned in children. Fluoroscopic evaluation may be required to determine whether actual rotatory fixation exists.
Anatomically, the C1-2 articulations are unique in the spine. The capsules surrounding the lateral C1-2 (facet) joints are relatively lax compared with other facet joints, whereas the ligaments surrounding the odontoid process such as the transverse, apical, and alar ligaments are relatively less compliant. Normally, the head can be rotated 90 degrees to the left and right, and one half of this rotation is made possible by the atlantoaxial articulations, the other one half allowed for by rotation of other cervical facet joints and the atlanto-occipital joints. The transverse ligament of the dens keeps the dens in close proximity to the anterior arch of C1, and the alar ligaments limit the extent of rotation of C1 relative to C2 from approximately 25 to 56 degrees. When hyper-rotational stress is placed on the C1-2 joints, rotatory subluxation can occur without disruption of the alar or other periodontoid ligaments. The alar ligaments are most resistant to dynamic loads placed on the C1-2 articulations.
The cause of the rotatory fixation is not always known but is believed to be related initially to swollen, redundant capsular and synovial tissues surrounding the lateral and anterior atlantoaxial articulations, secondary to inflammation or trauma. In many cases, there is no known etiology for AARF. In adults, this condition is often associated with severe degenerative disease of the upper cervical facets and may or may not be associated with torticollis ( Figs. 12-6 to 12-8 ) . Atlantoaxial rotatory fixation may be associated with anomalies of the atlanto-occipital or atlantoaxial articulations such as atlanto-occipital fusion ( Figs. 12-9 and 12-10 ) . In some cases, AARF occurs secondary to congenital maldevelopment of the ligaments adjacent to these articulations. In these cases, the involved ligaments become edematous, hyperemic, and lax, which predisposes them to AARF.





Concomitant muscle spasm may occur, especially in the acute post-traumatic setting. The muscle spasm usually involves the sternocleidomastoid muscle resulting in torticollis. Later on, capsular adhesions or contractures develop. The torn or thickened capsule may also invaginate into the lateral C1-2 (facet) joints, or meniscal-like synovial folds may form and extend into the lateral atlantoaxial (C1-2 facet) joints, thereby preventing or impairing rotational movement.
Atlantoaxial rotatory fixation has been classified into four types by Fielding :
Type 1. AARF without anterior displacement of the atlas. The odontoid acts as the pivot point (center of rotation). The transverse and alar ligaments of the dens are intact. (Most common type) (see Figs. 12-1 to 12-8 ).
Type 2. AARF with anterior displacement of the atlas by 3±5 mm. One articular mass acts as the pivot point. The transverse ligament is abnormal or deficient (second most common type) (see Figs. 12-9 and 12-10 ).
Type 3. AARF with anterior displacement of the atlas by greater than 5 mm. The transverse and alar ligaments are abnormal or deficient.
Type 4. AARF with posterior displacement of the atlas. (Rarest type associated with hypoplasia of the dens).
Rarely, a fifth type occurs in which both AARF and atlanto-occipital rotary subluxation are present. AARF may also occur in Grisel’s syndrome, which is nontraumatic atlantoaxial subluxation occurring after infection or surgery in the head and neck region, resulting in ligamentous laxity surrounding the atlantoaxial joints. Occasionally, the infected ligaments will rupture.
Patients with AARF present clinically with varying degrees of neck pain, diminished range-of-neck rotation, and the head is characteristically tilted, slightly flexed, and rotated to the side opposite the torticollis. Usually the patient has no neurologic deficit unless concomitant atlantoaxial subluxation is present. If there is hyper-rotation of the neck, the vertebral artery may be compromised.
Torticollis may occur with or without atlantoaxial rotatory fixation. Congenital anomalies of the sternocleidomastoid muscle (e.g., congenital fibrosis), painful neck conditions such as myositis, lymphadenitis, and tumors of the cervical spine may cause contraction of the sternocleidomastoid muscle, resulting in torticollis in the absence of AARF. These patients will have contraction of the sternocleidomastoid (SCM) muscle on the side opposite to the side the head is facing. In patients with both torticollis and AARF, the SCM muscle contraction occurs on the same side the head is facing. If torticollis does not resolve in 1 to 2 weeks, the diagnosis of AARF should be entertained. When atlantoaxial subluxation or AARF develops after prolonged involuntary neck posturing, an underlying diagnosis of dystonia should be considered.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


