Abstract
Bilateral renal agenesis is the congenital absence of both kidneys and ureters. Also known as Potter syndrome, it is a lethal anomaly in which absence of the kidneys results in lack of amniotic fluid and pulmonary hypoplasia, along with characteristic facies and positional extremity abnormalities. Fetal urine production is the major source of amniotic fluid production after 18 weeks’ gestation, and a lack of amniotic fluid after this gestational age supports the diagnosis. When the kidneys are absent, the adrenal glands fill the renal fossae bilaterally, and color Doppler imaging of the descending aorta fails to demonstrate either renal artery. Associated anomalies and aneuploidy are common. Bilateral renal agenesis is also a component of several genetic syndromes. First-degree relatives may be at increased risk for other renal anomalies.
Keywords
Potter syndrome, oligohydramnios sequence, lying-down adrenal sign
Introduction
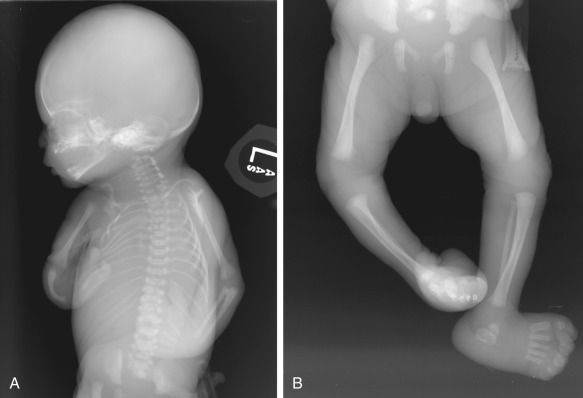
Bilateral renal agenesis is a uniformly lethal anomaly. Absence of the kidneys causes anhydramnios, resulting in pulmonary hypoplasia, characteristic facies, and positional extremity abnormalities ( Fig. 10.1 ). This constellation of findings was first described by Edith Potter, and bilateral renal agenesis has been termed Potter syndrome . The deformation sequence itself, which can occur following lack of amniotic fluid from any early insult (not merely from renal agenesis), is known as the oligohydramnios sequence or Potter sequence .
It is often challenging to diagnose absence of a structure, and bilateral renal agenesis can be particularly challenging because the lack of amniotic fluid impairs visualization. However, in population-based registries, renal agenesis has been diagnosed prenatally in about 90% of cases.
Disorder
Definition
Bilateral renal agenesis is the congenital absence of both kidneys and ureters.
Prevalence and Epidemiology
In Potter’s original series, the prevalence of bilateral renal agenesis was approximately 1 : 3000 births. In population-based studies involving routine prenatal ultrasound (US), the prevalence is 1 : 8000 to 1 : 9000 pregnancie s . The actual birth prevalence is less common because approximately two-thirds of pregnancies with bilateral renal agenesis are terminated.
Bilateral renal agenesis is three times more common in males. It is also more common in the setting of pregestational diabetes. Based on data from the National Birth Defects Prevention Study, obesity and cigarette smoking approximately double the risk for bilateral renal agenesis, and binge drinking in the second month may more than triple the risk.
Associated anomalies have been reported in a high percentage of cases, including VACTERL ( v ertebral, a nal, c ardiac, t racheal, e sophageal, r enal, and l imb anomalies; see Chapter 146 ) association in 48% and gastrointestinal atresia in 28%. Partial laterality defects have been identified in more than 50% of cases, including intestinal malrotation, incomplete lobulation of the right lung, and persistence of the left superior vena cava. Aneuploidy has been reported in 7%. Bilateral renal agenesis is also a component of several syndromes, including branchiootorenal syndrome, Fraser syndrome (see Chapter 128 ), and sirenomelia (see Chapter 144 ).
Etiology and Pathophysiology
Renal agenesis results when the ureteric bud either fails to develop from the mesonephric (Wolffian) duct or fails to induce the surrounding metanephric mesenchyme to form glomeruli and nephrons. There is usually absence of the seminal vesicles and vas deferens in males, and a high incidence of müllerian anomalies and müllerian agenesis in females.
There is a significant familial aggregation of cases, with a recurrence risk of 5% to 6% and an overall prevalence of renal anomalies of 15% among first-degree relatives. The RET (Rearranged in Transfection) tyrosine kinase signaling system appears to be critical for normal nephron size and function. In one series, about 30% of fetuses with bilateral renal agenesis had evidence of an RET gene mutation.
Manifestations of Disease
Clinical Presentation
The fundal height may lag behind gestational age because of lack of amniotic fluid. The prenatal diagnosis is based on US findings, as discussed subsequently.
Imaging Technique and Findings
Ultrasound.
Typically, the initial finding in the second trimester is a severe decrease or absence of the amniotic fluid volume. Fetal urine production is the major source of amniotic fluid after 16 to 18 weeks’ gestation. Whenever oligohydramnios is encountered, particularly in the second trimester, it is important to image the fetal renal fossae and pelvis. In bilateral renal agenesis, the kidneys are not present in either the renal fossae or in an ectopic pelvic location, and there is no urine visible in the bladder ( Fig. 10.2 ). However, the diagnosis may be challenging because lack of amniotic fluid can severely impair visualization.

When imaging the renal fossae, kidneys should be differentiated from the adrenal glands. The adrenal gland is suprarenal and almond-shaped, with a hypoechoic cortex and hyperechoic medulla. If a kidney is absent or in an ectopic location, the adrenal flattens and fills the fossa in what has been termed the “lying-down” adrenal sign ( Fig. 10.3 ). The adrenal is “lying down” on the psoas muscle, which is also hypoechoic.

Color Doppler imaging of the descending aorta is a useful adjunct because the renal arteries are reliably visualized when the kidneys are present, and they are absent in renal agenesis ( Fig. 10.4 ). The fetal abdomen is imaged in the coronal plane with the beam perpendicular to the aorta so that renal arteries arise at an angle of insonation below 20 degrees. If necessary, a nomogram is available to predict the location of the renal arteries, using the femur length as a reference.










