Fig. 12.1
Fifteen-year-old status posttrauma. Serial images from retrograde cystourethrogram (a, b) demonstrate extravasation of the contrast material secondary to a traumatic rupture in the bladder neck
Postvoid imaging of the UB is important because contrast extravasation may only be seen on postvoid images.
Ultrasound
Ultrasound is an attractive first-line imaging modality for trauma victims in emergency rooms, since it is a cheap, easily applicable, and reproducible noninvasive imaging modality.
Ultrasound is most useful for detection of fluid collections and confirmation of correct positioning of drainage catheters.
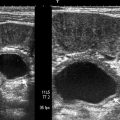
In extraperitoneal rupture, perivesical free fluid of variable echogenicity (usually hypoechoic) can be seen. The UB appears small and contracted, and the UB wall may appear thickened.
In cases of intraperitoneal rupture, free fluid is seen within the peritoneal cavity and the UB appears small and contracted.
Computed Tomography
Computed tomography (CT) has become accepted as the imaging modality of choice for patients with multiple injuries, and in light of recent developments in multidetector CT (MDCT) technology, CT is being more commonly used in emergency rooms for evaluation of trauma victims.
CT cystography can be used instead of conventional cystography as it allows faster and better anatomical evaluation of not only the UB but also the surrounding organs and bony pelvis.
CT cystography involves retrograde filling of the UB with 300–400 ml of (3–5 %) diluted nonionic contrast material and followed by acquisition of contiguous thin slice (5 mm) axial images through the pelvis.
Antegrade filling of the bladder by accumulation of intravenously injected contrast material is less reliable than retrograde filling, because it may not result in adequate UB distension, and may lead to a time loss of 15–30 min in the emergency setting.
CT cystography images obtained on an MDCT scanner can be easily reformatted in the sagittal and coronal planes (multiplanar reconstruction), allowing construction of lateral and oblique cystography images without additional radiation exposure and without moving the trauma victim with pelvic fractures.
The normal uninjured UB appears as a well distended hyper-attenuated structure within the pelvis, without perivesical fat stranding.
A classification system for UB injuries, based on cystographic patterns of extravasation in 97 trauma patients described by Sandler et al. in 1986, has been adapted for CT cystography and includes five types of UB injury:
Type 1: Bladder Contusion
A presumptive diagnosis of lower urinary tract injury (bladder or proximal urethra) in a patient with hematuria after blunt pelvic trauma but with normal findings at cystography. The exact nature of the injury is not known, but is not considered clinically to be a major injury.
Type 2: Intraperitoneal Rupture
Get Clinical Tree app for offline access
CT cystography demonstrates extravasated intraperitoneal contrast material around bowel loops and mesenteric folds (Figs. 12.2a–c, 12.3a–c, and 12.4a, b).
Fig. 12.2
Nineteen-year-old male patient with trauma history. (a) Contrast-enhanced axial CT image at upper abdomen level demonstrates significant hypodense fluid (arrow). (b) Axial CT image at pelvis level reveals contracted undistended urinary bladder and hemorrhagic free pelvic fluid (arrow). (c) Scanogram obtained on tomography table after retrograde urethral contrast administration demonstrates diffuse extravasation between intestinal loops consistent with intraperitoneal urinary bladder ruptureRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree