The organ most consistently and frequently affected by conventional cancer treatment is the bone marrow and secondarily the peripheral blood cells. The suppression of the stem cell in the marrow or the interference with the active proliferation of a particular cell line is predictable, based on the therapy modalities, chemotherapeutic agents, and radiotherapy modalities.
The depression of red blood cells, giving rise to anemia, occurs much more slowly than drug-induced leukopenia because of the differences in the half lives of the mature cells of these two cell lines. When one compares the half life of the red cell (˜120 days) with the half life of platelets (˜5-7 days) and with the half life of granulocytes (˜ 6-8 hours), it is evident why the latter two are more frequently involved in earlier and more severe suppression by chemotherapy and radiotherapy.
Table 24.1 Drug Class or Compound and Degree and Duration of Myelosuppression
If a particular agent predominantly affects the stem cells rather than cells in specific phases of the cell cycle, then all cell lines will be suppressed. Very few classes of chemotherapeutic agents selectively depress the stem cell. Examples of these agents are the general group of nitrosoureas (lomustine, carmustine). Other classes of agents, mainly the cell-cycle agents that are not specifically phase selective (such as the anthracyclines and certain alkylating agents like busulfan), may cause delayed suppression of bone marrow cells and longer recoveries than phase-specific agents like the antimetabolites and vinca alkaloids (Tables 24.1 and 24.2).
The degree of cytopenia is influenced by the age of the patient (children have a much more cellular marrow with a decreased percent of fat), stage of the disease, previous treatments, and the ability of the liver and kidney to metabolize and/or excrete the cytotoxic compound.
Nitrosoureas typically produce a late and often severe thrombocytopenia that occurs 4-6 weeks after the administration of the agent. Thrombocytopenia may occur after recovery from leukopenia and may persist for 1-2 weeks after the nadir occurs. Severe bone marrow hypoplasia may be seen after the administration of busulfan, which is used for conditioning in autologous bone marrow transplantation in pediatric solid tumors. Thrombocytopenia may persist long after the granulocyte count has returned to near normal values and is the last to recover. In leukemia, Cytosar causes severe aplasia with a transient blastema with circulating myeloblasts for a period of 1-7 days.
Generally, agents that are specifically cell-cycle active and phase-specific produce a rapid cytopenia (Table 24.2). Recovery is quicker, especially from agents that are active in S and M phases. Agents that tend to be non-cycle active or exert their effect in cells in G0 have the greatest delay myelosuppression and affect the stem cells before specific delineation in erythropoiesis, granulopoiesis, or megakaryopoiesis.
Very few cancer chemotherapy drugs are truly nonmyelosuppressive. Bleomycin, vincristine, and L-asparaginase generally do not cause significative bone marrow suppression.
HEMATOLOGICAL COMPLICATIONS OF RADIOTHERAPY
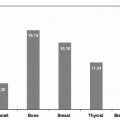
In adults, the head, cervical, thoracic, lumbar, and sacral spines account for approximately 13%, 3%, 14%, 11%, and 14% of the active bone marrow, respectively (1). In children, these values are different, reflecting the age-dependent distribution of functioning marrow. The long bones (femur, tibia), ribs, and skull, are hematopoietically more important in children than in adults.
Total body irradiation produces drastic decreases in leukocyte, erythrocyte, and platelet counts (1). The decrease in peripheral leukocyte count, especially lymphocyte count, following radiotherapy has been extensively reported in adult patients (2, 3, 4, 5). Plowman reported that lymphocyte counts remain depressed years after the radiation therapy (6). The decrease in erythrocytes is less spectacular and the erythropoietic system effectively compensates by proliferating upon demand (7). These effects of radiation on the hematopoietic system depend on several factors: pretreatment blood indices, stage of the cancer, the field location of treatment, surface area treated, the cumulative dose administered, as well as any other concurrent therapy received by the patient, especially chemotherapy (1,2,7, 8, 9).
Hematopoietic stem cells replicate and differentiate along lymphoid or myeloid lineages regulated by a network of hematopoietic growth factors and cellular interactions. Families of colony-stimulating factors have been identified that control the process of replication and differentiation. The hematopoietic system is also dependent on the microenvironment that consists of endothelial cells, adventitial cells, fibroblasts, macrophages, and fat cells (10).
The in vivo effects of localized single exposure to 250 kVp x-rays on the femoral bone marrow of rats demonstrated that doses of 10 Gy have transient effects on stromal function, and this is rapidly repaired (11). In contrast, doses of 20-100 Gy result in aplasia of the femur associated with extensive sinusoidal injury. Regeneration of bone marrow is performed by circulating pluripotent hematopoietic stem cells that disseminate to the locally aplastic segments of marrow and renew hematopoiesis. Some studies demonstrate that single-fraction doses of 5-10 Gy or fractionated irradiation to conventional fields such as mantle or pelvis delivering 1.8-2 Gy/day to 55-70 Gy at conventional dose rate produce decreased proliferative capacity of explanted stromal cells (12,13).
Table 24.2 Cell-Cycle Activity of Chemotherapeutic Agents