Nonmediastinal Injury
Chest trauma is directly responsible for 25% of all trauma deaths and is a major contributor in another 50% of all trauma mortality. Chest trauma may be blunt (90% of cases) or penetrating. Blunt thoracic injuries are the third most common injuries in polytrauma patients, following those of the head and extremity. Although 50% of blunt chest injuries are minor, 33% will require hospital admission. Rib fractures and pulmonary contusions are the most common injuries encountered. A chest radiograph is generally the first modality of radiologic evaluation of the chest trauma patient. It is essentially a screening examination and is used to identify life-threatening conditions such as a large hemothorax, tension pneumothorax, dangerously malpositioned lines and tubes, and mediastinal hematoma. Contrast-enhanced (CE) chest computed tomography (CT) is the gold standard for radiologic evaluation of the chest trauma patient. This chapter will review the spectrum of radiographic and CT imaging findings seen in patients sustaining major thoracic trauma, including the lungs, pleura, bones, and mediastinal structures.
Lung Injury
Pulmonary Contusion
Pulmonary contusions are the most common pulmonary injury and occur in 17% to 70% of blunt chest trauma patients, most commonly from motor vehicle collisions or falls from height. A pulmonary contusion results from injury to the alveolar wall and pulmonary vessels, allowing blood to leak into the alveolar and interstitial spaces of the lung. The causes are thought to include compression of the lung against the chest wall, shearing forces, rib fracture, or previously formed pleural adhesions tearing peripheral tissue as the lung separates from the chest wall at impact. Blast injuries also commonly cause pulmonary contusion.
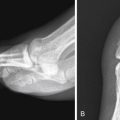
The appearance of pulmonary contusion on the chest radiograph depends on its severity. Minimal contusion may not be visible or may appear as an ill-defined area of patchy air space opacity ( Fig. 8-1 ). Severe contusion may appear as consolidation of a large area of lung ( Fig. 8-2 ). Air bronchograms may be seen in contused lung if there has not been filling of the airways with blood. Pulmonary contusion is typically nonsegmental and geographic, and it readily crosses pleural fissures, unlike pneumonia or atelectasis.


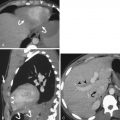
Compared with radiography, CT is much more sensitive in detection of pulmonary contusion ( Fig. 8-3 ). The appearance of pulmonary contusion may be delayed up to 6 hours on chest radiography but is seen immediately on chest CT. The CT appearance is similar to that of chest radiography. Minimal contusion may manifest as ground-glass density, often with subpleural sparing of 1 to 2 mm (especially in the pediatric population), often in the periphery of the lung or adjacent to bony structures such as the spine (see Fig. 8-3 ). On both radiography and CT, pulmonary contusion often “blossoms” in the first 24 to 48 hours after the injury as blood progressively accumulates in the lung parenchyma ( Figs. 8-4 and 8-5 ).



Contusions are a risk factor for development of pneumonia or acute respiratory distress syndrome. Patients with contusions seen only on the CT image and not on the chest radiograph may have a prognosis similar to those that do not have pulmonary contusions at all on CT (i.e., “CT-only” contusion may have a better outcome than contusions that are visible on both CT and chest x-ray examination). Pulmonary contusion usually resolves in 1 to 14 days ( Fig. 8-6 ). Generally, if the chest radiograph or CT has not cleared by day 14, alternate diagnoses such as development of pneumonia, acute respiratory distress syndrome, or aspiration should be considered.

Pulmonary Laceration
The mechanism of injury causing a pulmonary laceration is thought to be similar to that of pulmonary contusion: tearing of lung parenchyma due to compression, shearing forces, direct injury from rib fracture(s), or at the site of previously formed pleural adhesions. Pulmonary lacerations are round or oval in shape due to the elastic recoil of the lung ( Fig. 8-7 ). There may be single or innumerable lacerations with size ranging from a few millimeters to several centimeters in diameter ( Fig. 8-8 ). Air, blood, or both may fill in the laceration (see Fig. 8-5 ), and there will often be a thin pseudomembrane due to the compression of surrounding lung tissue. On the chest radiograph, pulmonary lacerations are often obscured for the first 48 to 72 hours because of surrounding pulmonary contusion (see Fig. 8-6 ). Computed tomography is much more sensitive in detection of pulmonary lacerations compared with radiography.


Active bleeding into a pulmonary laceration may occasionally be seen. On intravenous (IV) CECT active bleeding will appear as linear high density, with Hounsfield units (HU) similar to that of the aorta, within or adjacent to the laceration ( Fig. 8-9 ). A pulmonary laceration will typically take several weeks or months to resolve. During healing the laceration will gradually fill completely with blood and then gradually decrease in size ( Fig. 8-10 ). A blood-filled rounded healing pulmonary laceration could be mistaken for a pulmonary neoplasm if the history of relatively recent chest trauma is not known.


An uncommon complication of a pulmonary laceration is formation of a bronchopleural fistula. This condition is more likely to occur if the laceration is in the periphery of the lung, with only the thin pseudomembrane between it and the pleural space. Bronchopleural fistula should be suspected if there is a persistent pneumothorax, unrelieved by appropriately positioned single or multiple chest tubes. Rarely, a pulmonary abscess may complicate a pulmonary laceration.
Injuries Involving the Pleural Space
Pneumothorax
A pneumothorax is a collection of air in the pleural space. Air may enter the pleural space during trauma because of penetrating injury from a knife or gunshot, puncture from a fractured rib, rapid deceleration forces causing pulmonary laceration, or alveolar rupture from suddenly increased intrathoracic pressure at the time of impact.
The appearance of a pneumothorax on the chest radiograph will depend greatly on the patient position. The initial chest radiograph of the trauma patient is usually a supine film obtained in the emergency department or trauma bay. When the patient is in the supine position, air will collect in the anterior and medial aspects of the pleural space. On the chest radiograph this may manifest as increased lucency over the lower thorax/upper abdominal quadrant ( Figs. 8-11 and 8-12 ), a deep costophrenic angle sign ( Fig. 8-13 ), or a sharply defined border of the heart or diaphragm. The “double diaphragm” sign, seen when air in the pleural space outlines both the dome and the anterior insertion of the diaphragm, may also be identified. A thin lucency adjacent to the heart border may also be seen and represents air between the medial lung margin and the soft tissues of the mediastinum ( Fig. 8-14 ). In the upright patient a pneumothorax is typically seen as a thin, sharply defined line of the visceral pleura with no lung markings beyond this border ( Fig. 8-15 ).





There are numerous mimics of pneumothorax on chest radiography, including bullae, skin folds ( Fig. 8-16 ), bedding or clothing, and overlying tubes or catheters. Computed tomography is much more sensitive for detection of pneumothorax. It is estimated that up to 78% of pneumothoraces are missed by chest radiography.

Generally a chest tube is placed for all pneumothoraces seen on the supine chest radiograph or in any unstable patient with a potential pneumothorax. Occult pneumothorax, defined as a pneumothorax seen only on chest CT and not on the supine chest radiograph, is thought to occur in up to 15% of blunt chest trauma patients ( Fig. 8-17 ). Optimal management of the occult pneumothorax is currently debated. It was previously thought that an occult pneumothorax required a prophylactic chest tube because of risk for enlargement or development of tension pneumothorax, especially in patients on mechanical ventilation. There is growing evidence that a small occult pneumothorax can be safely managed in the majority of patients with close observation, without thoracostomy tube placement. About 10% of patients managed using this guideline will fail conservative management and ultimately require thoracostomy tube placement for symptomatic pneumothorax.

A tension pneumothorax occurs because of a one-way valve mechanism in which air can enter the pleural space but cannot get out. This results in rapid and progressive accumulation of air in the pleural space with increasing pressure causing contralateral shift of the mediastinum and compression of the vena cavae resulting in decreased cardiac output from impaired venous return ( Fig. 8-18 ). Note that tension pneumothorax is a clinical diagnosis but can be suggested by radiologic signs of increased lucency of the affected hemithorax, contralateral shift of the mediastinum, widened ipsilateral rib interspaces, depression of the ipsilateral hemidiaphragm, and lung collapse toward the hilum. Treatment is immediate decompression with chest tube thoracostomy. Rapid reexpansion of the lung after treatment of tension pneumothorax can lead to pulmonary edema. This occurs immediately after treatment of the pneumothorax and may be unilateral or bilateral. This condition occurs more commonly in patients 20 to 50 years of age. Although tension pneumothorax may be completely asymptomatic, there is a reported mortality rate of up to 20%. If there is persistent pneumothorax or air leak after chest tube placement, incorrect tube placement, bronchopleural fistula, or tracheobronchial injury should be suspected ( Fig. 8-19 ).


Hemothorax
Hemothorax is seen in 50% cases of blunt chest trauma. Sources of bleeding can be the intercostal arteries, thoracic spine, lung, great vessels, or heart. Hemothorax can also occur with hemoperitoneum and concurrent ruptured diaphragm.
On chest radiography at least 150 to 200 mL of blood are needed to detect pleural fluid on an upright chest radiograph. A meniscus sign is often seen with pleural fluid of any type and appears as a concave sloping of fluid in the costophrenic angle toward the lateral chest wall. A straight air-fluid level indicates hemopneumothorax. Because most trauma chest radiographs are performed with the patient in the supine position, blood will collect in the dependent portion of the thorax. A hemothorax will be seen on the supine film as a diffuse increase in density over the entire hemithorax. A dense rim of blood may be seen along the lateral lung margin as blood progressively fills the dependent pleural space and compresses the lung medially ( Fig. 8-20 ). A very large hemothorax can cause complete opacification of the affected hemithorax with contralateral shift of the mediastinum ( Fig. 8-21 ).


On CT, acute hemothorax is seen as hyperdense fluid in the dependent portion of the pleural space. Hounsfield units of acute hemorrhage will be higher than 15, generally in the range of 20 to 45 HU. Slightly higher density in the dependent portion of the hemothorax may be seen because of settling of blood products. As blood clots, the density of the blood increases to 50 to 90 HU. If there is intermittent bleeding in the pleural space, layers of different densities may be seen, constituting the “hematocrit effect.” Active bleeding within the pleural space will appear as a linear tract of high density (within 10 HU of the IV CE aorta) within the pleural space ( Fig. 8-22 ). Angiography with selective embolization may be used for treatment of active bleeding or pseudoaneurysm ( Fig. 8-23 ). The exact site of bleeding needs to be determined whether surgery or catheter embolization is the chosen treatment.


Simple or serous effusion, bile, chyle, and urine may also accumulate in the pleural space. A sympathetic serous effusion may be seen if there are injuries to the liver, spleen, or pancreas and will have HU density less than 15. Chylous effusion is due to an injury to the thoracic lymphatic duct and may have negative HU density because of the presence of fat. An effusion composed of bile or urine is seen with injury to the biliary or urinary system and a concurrent full-thickness diaphragm tear. Differentiating between bile and urine on CT can be very difficult and may require thoracentesis and analysis of fluid to establish the correct diagnosis ( Fig. 8-24 ). Delayed imaging of the renal collecting system may also be diagnostic if direct contrast leak is identified.

Extrapleural Hematoma
Extrapleural hematoma refers to blood that has collected between the parietal pleural and endothoracic fascia. The cause is usually a rib fracture that has lacerated an intercostal artery. On chest radiograph an extrapleural hematoma typically appears as a focal convex mass along the periphery of the lung. It may also be seen at the lung apex after subclavian vessel trauma or aortic injury ( Fig. 8-25 ). Unlike a pleural effusion or a hemothorax, an extrapleural hematoma will not change shape with a change in patient position. On CT an extrapleural hematoma appears as a fluid collection that causes inward displacement of the extrapleural fat ( Fig. 8-26 ). Active bleeding within the hematoma may be seen and can be treated with angiographic embolization.


Bony Thorax and Chest Wall
Soft Tissue Contusion
Soft tissue contusion or hematoma may be arterial or venous in origin. A hematoma from a high-pressure arterial injury may enlarge rapidly, whereas a hematoma from a low-pressure venous injury is usually self-limited. The trauma patient who is taking anticoagulants is at higher risk for developing a soft tissue contusion or hematoma from minor trauma.
On the chest radiograph a soft tissue contusion is not usually apparent unless there is a large amount of associated soft tissue hematoma. A large amount of hematoma may appear as increased density of the soft tissues or asymmetry of the soft tissues when compared to the uninjured side. Extensive soft tissue hematoma affecting one side of the chest wall can be hard to distinguish from a layering hemothorax on the supine chest radiograph. Excess soft tissues in an obese patient or a female patient with large breasts may mimic or obscure a chest wall hematoma.
The appearance of chest wall soft tissue trauma on CT will depend on the severity of the injury and can range from minimal fat stranding of the chest wall to a large hematoma with or without active bleeding ( Fig. 8-27 ). A seatbelt mark, identified as soft tissue bruising on the lower neck and center chest, is often seen in patients injured in motor vehicle collisions. The presence of a seat belt bruise or hematoma in the neck may be a marker for underlying cervical vessel injury, and a neck CT angiography may be warranted for further evaluation.

Rib Fractures
Rib fractures are the most common thoracic skeletal injury in blunt chest trauma, with an incidence of 50%. Rib fractures are most commonly the result of a motor vehicle collision in the adult patient. Rib fractures in older adults are most commonly due to falls. The lateral aspects of the ribs are the site most commonly fractured because of the chest wall architecture and decreased muscular support in this region. Chest radiography has sensitivity as low as 15% for detection of rib fractures. Computed tomography has a much higher sensitivity, especially when coronal reformatted images are reviewed.
Fractures of the eighth to eleventh ribs are associated with a higher incidence of injury to the spleen (left-sided fractures) or liver (right-sided fractures). When CT is obtained in the trauma patient with lower rib fractures, a routine search for injury involving these organs should be performed. Fractures of the first, second, and third ribs indicate high-velocity trauma and are associated with brachial plexus or subclavian vessel injury in 3% to 15% of blunt chest trauma patients. The rib number and site of each rib fracture should be specified in the radiology report because this provides prognostic information to the trauma surgeon. It has been shown that mortality increases 19% and pneumonia increases 27% in elderly patients with each additional rib fracture.
Flail chest, seen in 6% of blunt trauma patients, indicates the presence of at least two fractures in three or more consecutive ribs ( Fig. 8-28 ). Flail chest is associated with a mortality of 33%. The chest wall instability, paradoxical motion of the fractured segment, and invariable presence of underlying pulmonary contusion cause altered pulmonary mechanics that lead to atelectasis, stasis of secretions, and pneumonia. Recent research shows that open reduction and internal fixation of flail chest may lead to improved outcomes.

Sternal Fractures
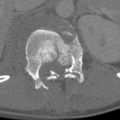
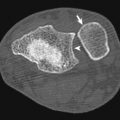
Sternal fractures are seen in 3% to 8% of blunt chest trauma patients. Fractures of the sternum are high-impact injuries. Motor vehicle collision is the most common cause, and the injury is usually due to the chest striking the steering wheel or the airbag impacting the chest wall. Sternal fractures are associated with rib fractures, cardiac contusion (1.5% to 6%), pericardial effusion, and cervicothoracic spine injuries. Although commonly associated with additional injuries, a nondisplaced sternal fracture can be seen as an isolated injury.
The supine chest radiograph will rarely demonstrate the fractured sternum unless the sternum is significantly displaced laterally. A properly exposed lateral chest radiograph, though rarely obtained in the acute trauma setting, will usually permit identification of at least mildly displaced fractures. Axial CT images will demonstrate most but not all sternal fractures. A clue on the axial CT images that there may be a sternal fracture is the anterior mediastinal or retrosternal hemorrhage that accompanies nearly all of these fractures. There will be a preserved fat plane between the posterior aspect of the retrosternal blood and the aorta ( Fig. 8-29 ). Traumatic aortic injury can also be a source of anterior mediastinal hemorrhage, but there will be no preserved fat plane and hemorrhage will be in direct contact with the aortic wall. Sagittal and coronal reformatted CT images are a significant aid in detection of a sternal fracture ( Figs. 8-30 and 8-31 ). Treatment is conservative in the vast majority of cases. Rarely, nonunion, severe pain, or sternal instability may require open reduction and internal fixation.



Mediastinal Injury
Tracheobronchial Injury
Tracheal and bronchial injuries from blunt trauma are rare. Actual full-thickness tears are more common in the thoracic than cervical segment and are associated with higher mortality. Most transbronchial tears occur close to the carina and more frequently on the right ( Fig. 8-32 ). Ruptures usually occur in the weaker posterior membranous portion. Mechanisms of the injury involve anterior-posterior compression of the chest forcing the lungs and mainstem bronchi laterally near the carina and exceeding the connective tissue strength of the airway, a sudden rise in intraluminal pressure when the glottis is closed, or by direct trachea crushing between the sternum and spine. The cervical portion can be sheared in rapid deceleration between the relatively immobile carina and cricoid and the more flexible trachea in between, by direct impact, or with sudden hyperextension and longitudinal traction. Tears typically occur across the weaker transverse plane. Injury can also result from a linear force applied across the cervical airway from a “clothesline” horizontal force when the neck impacts fixed linear obstacles like ropes, tree limbs, or wires ( Fig. 8-33 ).


The injury may be suggested by clinical signs/symptoms, including hemoptysis, cough, respiratory distress, cyanosis, subcutaneous air, hoarseness, aphonia/dysphonia from recurrent laryngeal nerve injury, and the Hamman “crunch” sign, when cardiac motion impacts adjacent mediastinal air. These findings are neither sensitive nor specific and may not be present with small or incomplete tears. Because of their rarity and other more overt coincident injuries, airway injuries are not suspected based on bedside findings and may be recognized only by imaging or when overt clinical complications arise.
Radiologic findings are more likely when there is positive pressure ventilator support. Air leaks into the mediastinum usually progress rapidly through tissue planes of the chest and beyond along fascial planes throughout the body. Pneumothorax can occur through dissection of air through the lung interstitium and visceral pleura, particularly from peripheral lung tears or through a direct tracheobronchial fistula ( Fig. 8-34 ). A finding suggesting a major airway-pleural communication is failure of a properly placed thoracostomy tube to relieve a simple or tension pneumothorax. When a major airway is breached, air enters the pleural space at the same rate it is evacuated by suction, maintaining the pneumothorax at constant pressure ( Fig. 8-35 ). Rarely an abrupt interruption or irregular tapering of the airway (bayonet sign) can be directly visualized radiographically. If there is a complete mainstem bronchial disconnection, the entire distal lung may collapse and fall into a gravity-dependent position (fallen lung; see Fig. 8-35 ). Airway interruption from blood clot or lacerated tissue occlusion will lead to persistent distal atelectasis.


If the cervical trachea is disrupted, an inflated endotracheal tube cuff may overexpand into the weakened or torn wall, producing an overdistended or caudally displaced balloon ( Fig. 8-36 ; see Fig. 8-32 ). A normally inflated balloon cuff is barely visualized radiographically. The course of the endotracheal tube may rarely deviate from the expected path of the trachea through a wall defect. Small portions of the balloon cuff may protrude/herniate through small tears.
The vast majority of blunt trauma patients with rapid onset and progressive mediastinal air leaks will NOT have injury to a major airway, but positive pressure respiratory support combined with lung laceration. Pneumomediastinum can be absent despite major airway injury when the adventitia remains intact or the tear is occluded by clot or an endotracheal tube balloon.

Computed tomography will display the same signs as chest radiographs with greater sensitivity and can detect airway tears directly ( Figs. 8-36 to 8-38 ). Major airway injuries can occur in association with clavicular, sternal, upper rib, and vertebral body extension fractures, but these are nonspecific indicators of airway injury and principally indicate a high level of impacting force. Concurrent major vascular injuries should be sought as indicated by mediastinal blood given the same chest compression or a shearing force mechanism of injury responsible for some cases of major airway disruption.
A large amount of mediastinal air around the trachea and mainstem bronchi does not indicate adjacent airway injury, but direct visualization of an airway-mediastinal connection is diagnostic.


The diagnosis of complete airway disruption can be supported by volumetric rendering, including endoluminal views (virtual bronchoscopy; see Figs. 8-32, 8-34, 8-37 ) or verified with bronchoscopy. Earlier diagnosis of this injury improves the chances for successful surgical airway repair, preserving pulmonary function, and preventing long-term complications of chronic airway narrowing.
Esophageal Injury
Esophageal injury sustained from blunt chest trauma is extremely rare. The injuries occur in the cervical and upper thoracic portions below the cricopharyngeal muscle and at the gastroesophageal junction, where there are transition points between relatively fixed and mobile segments. Not surprisingly, given the central protected location of the esophagus, injury typically requires high-force impacts and thus is likely to be accompanied by other thoracic injuries ( Fig. 8-39 ). Injury mechanisms include crushing between the impacted anterior chest wall and the spine, hyperextension of the spine mainly at the diaphragmatic hiatus, and laceration or entrapment related to fractures or dislocations of the thoracic spine ( Fig. 8-40 ). A sudden increase in intraesophageal pressure by compressive forces may also cause rupture. Injuries are typically in the proximal right posterior and distal left posterior portions. Radiographic signs of full-thickness injury are often absent early but could include pneumomediastinum, left pleural effusion, and abnormal mediastinal contour related to leakage of esophageal content or associated mediastinal hemorrhage. An atypical course of a nasogastric tube traversing a tear is another rare indirect radiologic finding.