Firearm-related injury is the second leading cause of death following motor vehicle collision. For every firearm death it is estimated that there are three to five other nonfatal firearm injuries. These injuries have become a major public health problem, creating a devastating impact on U.S. society with substantial emotional and financial cost. This chapter will describe the role of imaging in evaluating patients admitted with penetrating injuries to the abdomen and chest and the influence of imaging findings on management.
Ballistics
A missile exits the barrel of a weapon with significant kinetic energy. Military weapons and hunting rifles are high-energy weapons and have a muzzle velocity greater than 1000 ft/sec. Most civilian gunshot wounds (GSWs) result from medium-energy handguns, with a muzzle velocity less than 1000 ft/sec.
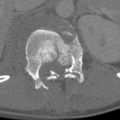
The extent of tissue damage caused by a projectile is more severe if the missile has high energy; yaws early in its path through tissue; is large in mass; hits bone, forming secondary missiles; or expands, deforms, or fragments when it strikes tissue. A permanent cavity results from the missile crushing the tissues it transits. The temporary cavity may enlarge from 20 to 25 times the diameter of the bullet fired from high-energy weapons. Severe damage results from the temporary cavity formation in fluid-filled organs (bladder or heart) and organs that have a dense parenchyma ( Fig. 12-1 ) (liver, kidney, brain). The temporary cavity formed from a medium-energy weapon (handgun) is insignificant and does not contribute significantly to the amount of tissue damage in far- or intermediate-range civilian GSWs.

Penetrating Injuries to the Torso
Mechanism of Injury
Most stab wounds are caused by knives, but they may also result from sharp objects or instruments. Unlike missiles, hand-driven low-energy weapons, such as a knife or ice pick, cause tissue damage only by their sharp cutting edge or point. Only 50% to 75% of victims of stabbing injuries to the anterior abdominal wall will have peritoneal penetration. Only 50% to 75% of these patients will have an injury that requires operative repair.
Unlike stab wounds, GSWs result in peritoneal penetration in 85% of abdominal gunshot wounds, and 80% of these patients will have significant organ injury. Surgeons use a penetrating abdominal trauma index (PATI) score to predict the severity of injury and risk for complications that occur following penetrating injuries. It takes into consideration the severity of the injury (1 minimal to 5 severe) to 14 organs and assigns a risk factor (1 to 5) for each organ. The PATI is obtained by multiplying the severity grade by the risk factor of all the injured organs and summing the individual organ scores. A high PATI score (>25) is typical of gunshot wounding and is associated with a higher likelihood of overtly positive peritoneal signs. Few, if any, further investigations are needed to confirm peritoneal violation.
Anatomic Regions
The torso (defined by the area between the internipple line and upper third of the thigh) is divided into five anatomic regions ( Fig. 12-2 ) to categorize the site of injury, as follows:
- 1.
The thoracoabdominal area defined by the internipple line superiorly, costal margins extended posteriorly, to the inferior tip of the scapula inferiorly.
- 2.
The anterior abdomen defined by the costal margins superiorly, anterior axillary lines laterally, inguinal ligaments and symphysis pubis inferiorly.
- 3.
The flank defined by the anterior and posterior axillary line (tip of the scapula superiorly and iliac crests inferiorly) and from the costal margin to the iliac crest.
- 4.
The back defined by the tips of the scapula superiorly and iliac crests inferiorly.
- 5.
The pelvis defined by the iliac crests and inguinal ligaments superiorly and upper thirds of the thighs inferiorly.


Mandatory Laparotomy
Before the mid-1960s it was believed that routine exploration for penetrating torso injuries would reduce mortality by 12% to 27% compared to expectant management. This concept arose from military experience since World War I. However, if such an approach were applied to all civilian penetrating injuries, 15% to 20% of GSWs and 35% to 53% of stab wounds to the torso would lead to an unnecessary (nontherapeutic) laparotomy.
Proponents of mandatory laparotomy based their belief on unproven assertions that intra-abdominal injury cannot be diagnosed short of exploration. They also believed that clinical examination was often unreliable in patients with serious injuries, that delay in diagnosis of these penetrating injuries would result in unacceptably high morbidity and mortality, and that nontherapeutic laparotomies were rarely associated with morbidity.
Indications for urgent laparotomy following penetrating trauma to the torso are shown in Box 12-1 . The standard of care in the United States for patients who are hemodynamically unstable or have overt clinical signs of peritonitis after sustaining gunshot or stab wounds is laparotomy. Other clear indications for immediate laparotomy include aspiration of frank blood via a nasogastric tube, evisceration of bowel, and bleeding from rectum on clinical examination, proctoscopy, or sigmoidoscopy. The availability of new surgical concepts and techniques and sophisticated new radiologic technology, the use of antibiotics, and recognition of the potential morbidity and increased hospital costs associated with laparotomy have challenged the dictum of mandatory exploration of the abdomen in the civilian setting.
Hemodynamic instability
Peritonitis
Bleeding from rectum
Aspiration of frank blood via nasogastric tube
Evisceration of bowel
Positive FAST findings
FAST , Focused assessment sonography for trauma.
Selective Conservative Management
The decision process of deciding which patient can be managed nonoperatively when there are no clear indications for surgery is termed selective conservative management . Over the past 4 decades, evidence of visceral injury has replaced simple peritoneal violation as the main indication for abdominal exploration. In the United States this policy is applied more often to stab wounds than GSWs in stable patients. Ideally a selective conservative approach should reduce the number of negative and nontherapeutic laparotomies without increasing the number, morbidity, or mortality of missed or delayed diagnoses of serious injuries.
The optimal method of ruling out peritoneal violation or significant visceral injury in hemodynamically stable patients with equivocal peritoneal signs following penetrating injury varies among institutions. The basic conservative management strategies, their strengths, and their weaknesses are listed in Table 12-1 . The anatomic location of the entry wound and the local practice at any given trauma center may dictate the management approach selected.
| Technique | Strength | Weakness |
|---|---|---|
| Serial clinical examination | Low NTLR, noninvasive | Physician, bed, and time intensive |
| Local wound exploration and DPL | Easy to perform; if negative, discharge patient; sensitive for intraperitoneal injury | Invasive; if positive, DPL has to be performed; cannot evaluate entry site to retroperitoneum and thoracoabdominal region; does not evaluate the retroperitoneum; no uniform agreement on the criteria for a positive lavage; high NTLR |
| Computed tomography | High sensitivity for peritoneal violation and organ injury, evaluates retroperitoneum | No uniform agreement for specificity for surgical intestinal injury, radiation |
| Ultrasonography (FAST) | High specificity for injury, easy to perform, noninvasive, no radiation | Low sensitivity for injury |
| Laparoscopy | High sensitivity for peritoneal violation and diaphragm injury | Requires a skilled operator, known to miss intestinal injury |
Management Strategies
Observation
Thirty-four percent to 72% of all patients with penetrating injury to the anterior abdomen or back are hemodynamically stable without overt signs of peritonitis and may be candidates for observation. The practice of observation with serial physical examination (ideally performed by the same examiner) can be accomplished safely, thereby reducing the number of nontherapeutic laparotomies. This technique could easily be performed on abdominal stab wounds. In the appropriate clinical setting this practice may also be applied to GSWs. The majority of patients with a reliable clinical examination who have minimal or no abdominal tenderness can be discharged after 24 hours of observation. Missed injuries requiring subsequent surgical exploration may occur in 4% to 6% of patients in the observation group, with an average delay in treatment ranging from 3 hours to 5 days. Compared to mandatory laparotomy, this management approach reduces the nontherapeutic laparotomy rate from 53% to 3% to 8%.
One disadvantage of observation with serial examination is the need for admission to the hospital for up to 72 hours because a significant amount of time may be needed for clinical signs of peritonitis to develop after perforation, especially if the injury involves the retroperitoneal colon or duodenum. In a busy trauma center or in a small community hospital, staff may not be available to perform frequent examinations. This limits the number of patients that can be regularly observed. Physical examination may be unreliable, and it may be difficult to elucidate signs of peritonitis in patients with associated severe head or spinal cord injuries, intoxication with alcohol or drugs, or other distracting injury.
Local Wound Exploration and Diagnostic Peritoneal Lavage
Local wound exploration and diagnostic peritoneal lavage (DPL) have been used to evaluate hemodynamically stable patients without peritonitis who are at risk for penetration of the peritoneum. A positive tap in blunt trauma is aspiration of 10 mL of blood. In penetrating trauma the definition of a positive tap is less clear. A tap is considered positive if feces, bile, or food material is aspirated through a catheter placed in the peritoneal cavity. A negative peritoneal tap is followed by a peritoneal lavage performed through the same catheter using 1 L of normal saline. The lavage effluent is sent for analysis. Local wound exploration is generally performed in the admission area under local anesthesia and sterile conditions. Local wound exploration is appropriate only for anterior abdominal stab wounds. It should not be used for gunshot wounds or stab wounds to the back or flank. If the peritoneum has not been violated, the exploration site is closed and the patient can be discharged following wound care. If there is penetration of the peritoneum or if wound exploration is equivocal for peritoneal violation, DPL may then be performed to assess for intraperitoneal injuries.
There is no uniform agreement among surgeons on the peritoneal lavage red blood cell (RBC) count that is an appropriate trigger for exploration. Currently the number of RBCs per cubic millimeter sufficient to perform surgical exploration ranges from 1000 to 100,000/mm 3 ; it varies among trauma centers and is based on the injury mechanism ( Table 12-2 ). The lavage technique is highly sensitive when based on low RBC counts and highly specific using high RBC counts.
| Mechanism of Injury | RBC Count (RBCs/mm 3 ) | Sensitivity | Specificity |
|---|---|---|---|
| SW | 5000 | 100% | 0% |
| SW | 50,000 | 94%-96% | 75%-88% |
| SW | 100,000 | 76% | 75% |
| GSW | 100,000 | 100% | 71% |
Significant injuries to the diaphragm and small bowel may occur with minimal hemorrhage and can be associated with false-negative DPL results. The inability to define the anatomic source of hemorrhage or severity of injury by DPL may increase the rate of nontherapeutic laparotomies in nonbleeding solid visceral injuries. Because DPL does not survey the retroperitoneum, it is unreliable in evaluating retroperitoneal organ injury and should not be used as the sole technique in the evaluation of patients with penetrating injuries to the flank and back. Local wound exploration may be difficult in obese patients, patients with thick back muscles, penetration in the thoracoabdominal region, or the presence of a large actively bleeding abdominal wall hematoma.
To improve patient flow, busy trauma centers prefer local wound exploration and DPL to observation with serial physical examination in order to triage asymptomatic patients with penetrating torso injury. Patients that have a DPL should be admitted for 24 hours to screen for any DPL complication and/or missed gastrointestinal injury. Unlike serial physical examination that warrants admission of a large number of patients for up to 3 days, these techniques can immediately eliminate patients who need not be observed. Intraperitoneal injuries in asymptomatic patients are also more likely to be detected acutely. This approach eliminates the risk for potential morbidity and mortality associated with a delay in injury diagnosis.
Multidetector Computed Tomography
Currently, triple-contrast multidetector computed tomography (MDCT) has become a valuable imaging modality to evaluate penetrating trauma to the torso considered for nonoperative management immaterial of the entry site or the number of gunshot or stab wounds. In this group of patients, MDCT can be very helpful and accurate in facilitating management decisions. Oral and intravenous contrast is also used routinely to optimize the detection of injuries to the intraperitoneal bowel, solid organs, mesentery, retroperitoneal genitourinary system, and duodenum. Penetrating trauma to the flank and back in asymptomatic patients is rarely associated with injury to critical retroperitoneal viscera because these organs are well protected by ribs, the spine, and the large back and paraspinal muscles. Patients with isolated retroperitoneal injuries resulting from these two anatomic locations may not present with overt clinical signs or symptoms and are not evaluated by DPL. It is important to routinely use rectal contrast material to opacify the entire colon to demonstrate contrast extravasation or focal colonic wall thickening, which enhances the ability to diagnose subtle colonic injuries that require surgical repair. Fifty-eight percent of patients with penetrating trauma to the back or flank incur intraperitoneal injuries. Combined intraperitoneal and retroperitoneal injuries may occur in about 16% of these patients.
Triple-contrast MDCT is highly sensitive and accurate in excluding peritoneal violation in patients with penetrating torso trauma. Among patients with peritoneal violation, MDCT has a high specificity, positive predictive value, and accuracy in predicting the need for laparotomy. It also helps to diagnose isolated liver injury, allowing nonoperative management for patients with penetration limited to the right upper quadrant.
Typically triple-contrast MDCT results are classified into negative, minor, or low risk for injuries and major or high risk for injuries. Patients with minor or low-risk injuries (small retroperitoneal hematoma or minor renal injury) are generally managed conservatively. Patients with major injuries are managed with surgery or angiography. In a busy trauma center, triple-contrast spiral MDCT is a safe and reliable technique to triage stable patients with penetrating injuries to the torso with no clinical or radiographic signs of peritoneal violation.
Diagnostic Laparoscopy
Laparoscopy enables direct visualization of the peritoneum and the intraperitoneal viscera to diagnose peritoneal violation and evaluate potential organ injury. Typically the diagnostic laparoscopy is converted to a laparotomy in the presence of peritoneal violation, major organ injury, or significant hematoma. Patients with no peritoneal penetration or with nonbleeding solid organ injuries may be observed or discharged. Laparoscopy still carries a 17% to 20% rate of nontherapeutic laparotomy and 17% negative laparotomy rate. Laparoscopy can prevent unnecessary laparotomies in 34% to 60% of patients with a concurrent reduction in hospitalization duration and costs.
The strength of diagnostic laparoscopy appears to be in the evaluation of patients with penetrating injuries to the left thoracoabdominal area with potential for small diaphragmatic rents. Local wound exploration is unreliable and associated with the risk for creating a pneumothorax. Laparoscopy reduces the number of nontherapeutic laparotomies, as compared to DPL, that may be performed among the subset of patients with minor splenic and liver injuries that have stopped bleeding by the time of surgery. Laparoscopy has also been shown to be optimally suited to evaluate the diaphragm for injuries in asymptomatic patients with less than 10,000 RBCs/mm 3 in the DPL effluent.
The limitations of laparoscopy include the need for general anesthesia and inadequate visualization of the retroperitoneum. Laparoscopy may also miss gastrointestinal injuries. The sensitivity can be as low as 18% for diagnosing bowel injury following penetrating trauma to the abdomen.
Tension pneumothorax may develop during laparoscopy in patients with diaphragm injury, and special precautions should be taken to avoid this complication. One major contraindication for laparoscopy includes prior history of multiple adhesions and patients with elevated intracranial pressure, who may suffer adverse effects from the insufflation of carbon dioxide. A significant cost savings will be gained only if laparoscopy is performed under local anesthesia.
Ultrasonography
There has been little enthusiasm to embrace ultrasonography as an initial screening study to evaluate patients with penetrating trauma to the torso. Though ultrasound can demonstrate free intraperitoneal fluid in blunt trauma patients, these results have not been reproduced in patients suffering penetrating injuries to the abdomen. The overall sensitivity of focused assessment sonography for trauma (FAST) to detect free fluid in the peritoneal cavity (in the perisplenic, perihepatic, pelvic, and pericardial spaces) is 47%. Ultrasonography is typically used only to detect free fluid. A significant number of patients with negative FAST study results have serious abdominal injuries requiring surgical repair. Positive FAST results are a strong predictor of intra-abdominal injury (specificity of 94%, positive predictive value of 90%). Thus positive FAST results should prompt immediate exploration.
Management Strategies
Observation
Thirty-four percent to 72% of all patients with penetrating injury to the anterior abdomen or back are hemodynamically stable without overt signs of peritonitis and may be candidates for observation. The practice of observation with serial physical examination (ideally performed by the same examiner) can be accomplished safely, thereby reducing the number of nontherapeutic laparotomies. This technique could easily be performed on abdominal stab wounds. In the appropriate clinical setting this practice may also be applied to GSWs. The majority of patients with a reliable clinical examination who have minimal or no abdominal tenderness can be discharged after 24 hours of observation. Missed injuries requiring subsequent surgical exploration may occur in 4% to 6% of patients in the observation group, with an average delay in treatment ranging from 3 hours to 5 days. Compared to mandatory laparotomy, this management approach reduces the nontherapeutic laparotomy rate from 53% to 3% to 8%.
One disadvantage of observation with serial examination is the need for admission to the hospital for up to 72 hours because a significant amount of time may be needed for clinical signs of peritonitis to develop after perforation, especially if the injury involves the retroperitoneal colon or duodenum. In a busy trauma center or in a small community hospital, staff may not be available to perform frequent examinations. This limits the number of patients that can be regularly observed. Physical examination may be unreliable, and it may be difficult to elucidate signs of peritonitis in patients with associated severe head or spinal cord injuries, intoxication with alcohol or drugs, or other distracting injury.
Local Wound Exploration and Diagnostic Peritoneal Lavage
Local wound exploration and diagnostic peritoneal lavage (DPL) have been used to evaluate hemodynamically stable patients without peritonitis who are at risk for penetration of the peritoneum. A positive tap in blunt trauma is aspiration of 10 mL of blood. In penetrating trauma the definition of a positive tap is less clear. A tap is considered positive if feces, bile, or food material is aspirated through a catheter placed in the peritoneal cavity. A negative peritoneal tap is followed by a peritoneal lavage performed through the same catheter using 1 L of normal saline. The lavage effluent is sent for analysis. Local wound exploration is generally performed in the admission area under local anesthesia and sterile conditions. Local wound exploration is appropriate only for anterior abdominal stab wounds. It should not be used for gunshot wounds or stab wounds to the back or flank. If the peritoneum has not been violated, the exploration site is closed and the patient can be discharged following wound care. If there is penetration of the peritoneum or if wound exploration is equivocal for peritoneal violation, DPL may then be performed to assess for intraperitoneal injuries.
There is no uniform agreement among surgeons on the peritoneal lavage red blood cell (RBC) count that is an appropriate trigger for exploration. Currently the number of RBCs per cubic millimeter sufficient to perform surgical exploration ranges from 1000 to 100,000/mm 3 ; it varies among trauma centers and is based on the injury mechanism ( Table 12-2 ). The lavage technique is highly sensitive when based on low RBC counts and highly specific using high RBC counts.
| Mechanism of Injury | RBC Count (RBCs/mm 3 ) | Sensitivity | Specificity |
|---|---|---|---|
| SW | 5000 | 100% | 0% |
| SW | 50,000 | 94%-96% | 75%-88% |
| SW | 100,000 | 76% | 75% |
| GSW | 100,000 | 100% | 71% |
Significant injuries to the diaphragm and small bowel may occur with minimal hemorrhage and can be associated with false-negative DPL results. The inability to define the anatomic source of hemorrhage or severity of injury by DPL may increase the rate of nontherapeutic laparotomies in nonbleeding solid visceral injuries. Because DPL does not survey the retroperitoneum, it is unreliable in evaluating retroperitoneal organ injury and should not be used as the sole technique in the evaluation of patients with penetrating injuries to the flank and back. Local wound exploration may be difficult in obese patients, patients with thick back muscles, penetration in the thoracoabdominal region, or the presence of a large actively bleeding abdominal wall hematoma.
To improve patient flow, busy trauma centers prefer local wound exploration and DPL to observation with serial physical examination in order to triage asymptomatic patients with penetrating torso injury. Patients that have a DPL should be admitted for 24 hours to screen for any DPL complication and/or missed gastrointestinal injury. Unlike serial physical examination that warrants admission of a large number of patients for up to 3 days, these techniques can immediately eliminate patients who need not be observed. Intraperitoneal injuries in asymptomatic patients are also more likely to be detected acutely. This approach eliminates the risk for potential morbidity and mortality associated with a delay in injury diagnosis.
Multidetector Computed Tomography
Currently, triple-contrast multidetector computed tomography (MDCT) has become a valuable imaging modality to evaluate penetrating trauma to the torso considered for nonoperative management immaterial of the entry site or the number of gunshot or stab wounds. In this group of patients, MDCT can be very helpful and accurate in facilitating management decisions. Oral and intravenous contrast is also used routinely to optimize the detection of injuries to the intraperitoneal bowel, solid organs, mesentery, retroperitoneal genitourinary system, and duodenum. Penetrating trauma to the flank and back in asymptomatic patients is rarely associated with injury to critical retroperitoneal viscera because these organs are well protected by ribs, the spine, and the large back and paraspinal muscles. Patients with isolated retroperitoneal injuries resulting from these two anatomic locations may not present with overt clinical signs or symptoms and are not evaluated by DPL. It is important to routinely use rectal contrast material to opacify the entire colon to demonstrate contrast extravasation or focal colonic wall thickening, which enhances the ability to diagnose subtle colonic injuries that require surgical repair. Fifty-eight percent of patients with penetrating trauma to the back or flank incur intraperitoneal injuries. Combined intraperitoneal and retroperitoneal injuries may occur in about 16% of these patients.
Triple-contrast MDCT is highly sensitive and accurate in excluding peritoneal violation in patients with penetrating torso trauma. Among patients with peritoneal violation, MDCT has a high specificity, positive predictive value, and accuracy in predicting the need for laparotomy. It also helps to diagnose isolated liver injury, allowing nonoperative management for patients with penetration limited to the right upper quadrant.
Typically triple-contrast MDCT results are classified into negative, minor, or low risk for injuries and major or high risk for injuries. Patients with minor or low-risk injuries (small retroperitoneal hematoma or minor renal injury) are generally managed conservatively. Patients with major injuries are managed with surgery or angiography. In a busy trauma center, triple-contrast spiral MDCT is a safe and reliable technique to triage stable patients with penetrating injuries to the torso with no clinical or radiographic signs of peritoneal violation.
Diagnostic Laparoscopy
Laparoscopy enables direct visualization of the peritoneum and the intraperitoneal viscera to diagnose peritoneal violation and evaluate potential organ injury. Typically the diagnostic laparoscopy is converted to a laparotomy in the presence of peritoneal violation, major organ injury, or significant hematoma. Patients with no peritoneal penetration or with nonbleeding solid organ injuries may be observed or discharged. Laparoscopy still carries a 17% to 20% rate of nontherapeutic laparotomy and 17% negative laparotomy rate. Laparoscopy can prevent unnecessary laparotomies in 34% to 60% of patients with a concurrent reduction in hospitalization duration and costs.
The strength of diagnostic laparoscopy appears to be in the evaluation of patients with penetrating injuries to the left thoracoabdominal area with potential for small diaphragmatic rents. Local wound exploration is unreliable and associated with the risk for creating a pneumothorax. Laparoscopy reduces the number of nontherapeutic laparotomies, as compared to DPL, that may be performed among the subset of patients with minor splenic and liver injuries that have stopped bleeding by the time of surgery. Laparoscopy has also been shown to be optimally suited to evaluate the diaphragm for injuries in asymptomatic patients with less than 10,000 RBCs/mm 3 in the DPL effluent.
The limitations of laparoscopy include the need for general anesthesia and inadequate visualization of the retroperitoneum. Laparoscopy may also miss gastrointestinal injuries. The sensitivity can be as low as 18% for diagnosing bowel injury following penetrating trauma to the abdomen.
Tension pneumothorax may develop during laparoscopy in patients with diaphragm injury, and special precautions should be taken to avoid this complication. One major contraindication for laparoscopy includes prior history of multiple adhesions and patients with elevated intracranial pressure, who may suffer adverse effects from the insufflation of carbon dioxide. A significant cost savings will be gained only if laparoscopy is performed under local anesthesia.
Ultrasonography
There has been little enthusiasm to embrace ultrasonography as an initial screening study to evaluate patients with penetrating trauma to the torso. Though ultrasound can demonstrate free intraperitoneal fluid in blunt trauma patients, these results have not been reproduced in patients suffering penetrating injuries to the abdomen. The overall sensitivity of focused assessment sonography for trauma (FAST) to detect free fluid in the peritoneal cavity (in the perisplenic, perihepatic, pelvic, and pericardial spaces) is 47%. Ultrasonography is typically used only to detect free fluid. A significant number of patients with negative FAST study results have serious abdominal injuries requiring surgical repair. Positive FAST results are a strong predictor of intra-abdominal injury (specificity of 94%, positive predictive value of 90%). Thus positive FAST results should prompt immediate exploration.
Imaging of Penetrating Torso Trauma
Radiography
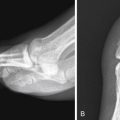
Radiographs are the initial imaging modality performed to localize a bullet and to evaluate for peritoneal violation. To determine the missile caliber from radiographs, the bullets should be seen on two views with no deformity, and the degree of magnification should be taken into account. Localization of a bullet or penetrating foreign body needs two radiographs obtained at 90 degrees or tomographic images ( Fig. 12-3 ). Occasionally these two views may not be able accurately localize the exact site of the penetrating object ( Figs. 12-4 to 12-6 ). It would be extremely risky to determine the course of a penetrating object using radiographs, by extrapolating a straight line between the entry and exit wounds or between the bullet and the entry site (see Fig. 12-3 ). Missiles do not take the shortest path between two points because the assailant may have been in motion when the injury occurred and missiles traveling through tissue with different density can change course.




Typically, trauma centers routinely obtain a chest radiograph and two views (anteroposterior [AP] and lateral projections) of the abdomen, usually performed without moving the patient ( Fig. 12-7 ). Chest radiographs can be obtained in patients with penetrating trauma to the torso because penetrating injuries of the upper abdominal and thoracoabdominal regions are associated with thoracic pathologic conditions and need to be assessed for pneumoperitoneum. If feasible, chest radiographs should be obtained in the erect position to increase sensitivity for the detection of pneumoperitoneum. These three views help to evaluate for peritoneal penetration and localize the penetrating object. Localized views may be required in obese patients or in regions of dense structure such as the pelvis ( Figs. 12-8 and 12-9 ) to localize the penetrating object or evaluate for fractures. Radiographic findings of peritoneal violation include an intraperitoneal bullet (see Figs. 12-7 and 12-8 ) or a penetrating object and pneumoperitoneum ( Figs. 12-10 and 12-11 ). Displacement of intraperitoneal organs by hematomas may help to localize the site and extent of injury. Abdominal and chest radiographs have a low sensitivity and lack specificity for intra-abdominal injuries (see Figs. 12-3, 12-8, and 12-11 ). The erect chest radiograph is positive for pneumoperitoneum in only approximately 18% of patients with surgically proven intestinal perforation.





Computed Tomography
Multidetector CT is the imaging modality of choice to evaluate patients who are hemodynamically stable following blunt trauma and has been shown during the last 2 decades to be accurate in diagnosing solid organ and hollow viscus injury. In the setting of penetrating trauma, MDCT is both far more sensitive and specific than radiography for identifying injuries to organs along a wound track. Multidetctor CT is currently a popular diagnostic modality in hemodynamically stable patients with penetrating injuries to the torso without radiographic or clinical signs of peritonitis to detect peritoneal violation and intraperitoneal and retroperitoneal injuries. Contraindications for MDCT are listed in Box 12-2 .
Hemodynamic instability
Peritonitis
Bleeding from rectum
Aspiration of frank blood via nasogastric tube
Evisceration of bowel
Positive FAST findings
FAST , Focused assessment sonography for trauma.
Technique
Triple-contrast MDCT scans are obtained from the internipple line to the symphysis pubis following administration of intravenous, rectal, and oral contrast material. The computed tomography (CT) parameters used at our institution for multislice spiral CT and for administration of intravenous contrast material are discussed in Chapter 11 . A total volume of 600 mL of 2 % sodium diatrizoate (Hypaque) oral contrast material is administered 30 minutes before and immediately before initiation of the scan. An enema of 1 to 1.5 L of 2 % sodium diatrizoate is also administered on the CT table to opacify the colon before scanning. Delayed images are obtained routinely in the portal venous phase or at about 3 minutes following injection of intravenous contrast material to evaluate the renal collecting system.
Active Bleeding, Hemoperitoneum, and Free Fluid
Multidetctor CT is extremely sensitive in detecting even small quantities of free intraperitoneal fluid or hemoperitoneum. Using attenuation measurements of free intraperitoneal fluid seen within the peritoneal cavity, CT is able to distinguish between free fluid, blood, hematoma, bile, and active bleeding ( Figs. 12-12 and 12-13 ). On contrast-enhanced CT scans, free intraperitoneal fluid measures between 0 and 15 HU, free blood between 20 and 40 HU, clotted blood or hematoma between 40 and 70 HU, and active bleeding not less than 10 HU of the attenuation of intravenous contrast material seen within an adjacent major artery.


The significant difference in the attenuation value of extravasated contrast material (range, 85 to 350 HU; mean, 132 HU) and hematoma (range, 40 to 70 HU; mean, 51 HU) is helpful in differentiating active bleeding from clotted blood (see Figs. 12-12 and 12-13 ). This attenuation difference between clotted blood and active bleeding may often be appreciated on inspection and without need for measuring attenuation values using a region of interest.
The extended areas that can be scanned to obtain high-resolution imaging by MDCT during various phases (arterial, portal venous, and excretory) of intravenous contrast material administration help to better demonstrate active bleeding compared to conventional or spiral CT. On MDCT, ongoing hemorrhage may be seen as an increase in the amount of intravenous contrast material extravasated on images obtained in the identical anatomic region during dual-phase imaging ( Fig. 12-14 ). Using MDCT scanners with greater than 40 slices with dual-phase imaging (arterial and portal venous phase), active bleeding may be seen only on the portal venous phase (see Fig. 12-14 ). This typically occurs when faster scanners outrun the vascular contrast bolus, especially when there is slow bleeding, bleeding from peripheral small arterial branches, venous hemorrhage, or vascular spasm. Blood and fluid show lower attenuation compared to the contrast-enhanced parenchyma of solid organs (see Figs. 12-12 to 12-14 ). Blood appears hyperattenuating compared to the parenchyma on unenhanced CT ( Fig. 12-15 ). Blood or hematoma may appear isodense to suboptimally enhancing parenchyma, making it difficult to visualize by CT (see Fig. 12-14 ). To avoid this pitfall it is important to scan during peak parenchymal enhancement (portal venous phase) and to administer an adequate volume and concentration of intravenous contrast material based on patient body habitus. Bolus-tracking techniques and using a saline flush to use all the contrast material injected can be helpful to achieving peak arterial parenchymal enhancement without use of an excessive amount of contrast material. Oral and rectal contrast material to opacify the small bowel and the entire colon should also be administered routinely. This contrast helps demonstrate subtle bowel wall thickening ( Fig. 12-16 ) and distinguish small quantities of intramesenteric blood, fluid, or hematoma from aggregated nonopacified bowel loops that can mimic these findings. Extravasation of a subtle amount of enteric contrast material may be the only specific finding of a surgical bowel injury ( Fig. 12-17 ; see Fig. 12-16 ).




Small amounts of blood or free fluid are typically seen in the most gravity-dependent regions of the peritoneal cavity. In the supine position the most dependent region of the peritoneal cavity is the hepatorenal fossa (Morison pouch) (Fig. 20-18). Other areas where free fluid or blood is often seen in trauma patients are the pelvis between the sigmoid colon and the bladder, the paracolic gutters, and the perihepatic and perisplenic spaces (see Figs. 12-1, 12-5, and 12-11 ). Careful inspection of these areas is necessary to identify small quantities of fluid or blood that may be the only CT sign of peritoneal violation, a subtle or occult intraperitoneal visceral injury (see Figs. 12-5, 12-8, and 12-18 ). Measuring the attenuation value of the free intraperitoneal blood in the various anatomic locations in the peritoneal cavity is important because the highest-attenuation blood will be seen adjacent to the injured organ and this is referred to as the sentinel clot ( Fig. 12-19 ). This CT sign is reliable and helpful in localizing the source of hemorrhage when evaluating MDCT in patients with hemoperitoneum in multiple compartments or with multiple visceral injuries.

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


