Clinical Reasoning
• In most cases—for women under 30 and for lactating and pregnant women—breast sonography has become the first phase of imaging for evaluating palpable masses. Breast sonography, however, is not recognized as a screening study for microcalcifications.
• Breast sonography is generally performed to determine the composition or characterization of a localized lesion(s) (that may or may not be palpable) and to further evaluate mammographic and clinical findings.
• Additional indications for breast sonography include ultrasound-guided biopsies, treatment plans for radiation therapy, and evaluating complications associated with breast implants.
• In some cases, whole-breast scanning may be recommended for diffuse diseases, such as fibrocystic disease.
Overview
Anatomy
• Each breast lies anterior to the sixth rib, pectoralis major, serratus, and external oblique muscles. The second and third ribs form the superior border of each breast and the seventh costal cartilage is the inferior border. The medial border of each breast is the sternum and laterally the breasts are bound by the margin of the axilla. The most anterior aspect of the breast is attached to the skin.
• Breast tissue is supported by Cooper’s ligaments, suspensory ligaments that extend posteriorly from the deep muscle fascia, through the breast, to the skin.
• The breast is comprised of:
• Parenchymal elements (lobes, ducts, and alveoli).
• Stromal elements (connective tissue and fat).
• The breast is described in terms of 3 layers:
1. Subcutaneous layer: Skin and subcutaneous fat lobules.
2. Mammary layer: 15 to 20 lobes that contain alveoli (multiple glandular tissue lobules), and ducts that drain to the nipple; fat lobules, and connective tissue.
3. Retromammary layer: Fat lobules and connective tissue.
Physiology
• The breasts or mammary glands are exocrine glands (release secretions through ducts) whose primary function is lactation (the secretion of milk) through lactiferous ducts (ducts in breast parenchyma) following pregnancy.
Sonographic Appearance
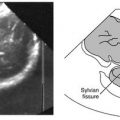
• As shown in the image on the facing page, the 3 layers of the breast are sonographically distinguishable; their normal appearance is described as follows:
1. The subcutaneous layer is the most anterior layer bordered anteriorly by the bright skin line and posteriorly by the mammary layer. In between, the subcutaneous fat lobules appear as low-level echoes with bright margins.
2. The mammary layer is the middle layer of the breast that contains glandular tissue or breast parenchyma. Typically it appears hyperechoic compared to the subcutaneous and retromammary layers due to its mixed parenchymal appearance depending on the amount of fat that is present:
• The appearance with the presence of little fat is highly echogenic due to the reflective appearance of the existing connective tissue (collagen and fibrotic tissue).
• When fat is present, the appearance is of areas of low-level echoes (fat) mixed with areas of high echogenicity (connective tissue). When visualized, the ducts appear as small anechoic branches running throughout the layer.
3. The retromammary layer is generally hypoechoic relative to the mammary layer and hyperechoic compared to the posterior border, the pectoralis major muscle (large chest muscle), which has a low- to very low–level echo texture.

• Although all the breast layers are influenced by the age of the woman and the functional state of the breast, the mammary layer shows the greatest changes sonographically.
• The sonographic appearance of the breast changes with age.
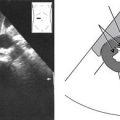
• The breasts of young women contain a high percentage of parenchymal elements and little fat. This causes the breast to be dense and appear highly echogenic.

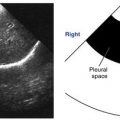
• The next image demonstrates the thin, linear, bright appearance of Cooper’s ligament. Notice how the ligament appears hyperechoic relative to adjacent structures.

Normal Variants
• Fatty breast: Increased fatty components throughout the breast resulting from age, parity, and menopause. When fat is present, the sonographic appearance is areas of low level echoes (fat) mixed with areas of high echogenicity (connective tissue surrounding mammary ducts).
• Fibrocystic breast: Commonly found in women of childbearing age. Fibrous tissues and cystic areas occur throughout the breast, as well as an increase in the amount of dense connective tissue, which will cause the breast to appear highly echogenic.
Preparation
Patient Prep
• None.
Transducer
• 10 to 18 MHz linear.
• Use compression sonography when assessing fibrocystic breasts.
Patient Position
Patient Position for Breast Lesion Scanning
• Position the patient to minimize the thickness of the portion of the breast being evaluated.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


