Overview
Location
• The liver occupies the right side of the upper abdomen and often extends beyond the midline of the body to the left side. Generally, it lies between the level of the nipples to the level of the eighth or ninth rib.
• Except for a bare area that encompasses most of the liver’s posterior surface, it is intraperitoneal (enclosed in the sac formed by the parietal peritoneum). Additional interruptions of the peritoneum at the liver include the gallbladder fossa, porta hepatis (the area of the hilus/opening where the portal vein and hepatic artery enter the liver and the common duct exits), falciform ligament attachment, and portions around the inferior vena cava (IVC).
• The liver is the most anterior visceral organ of the peritoneal cavity. The left lobe and majority of the right lobe are surrounded by the rib cage. The remaining portion of the right lobe is usually in contact with the abdominal wall.
• Superior, posterior, and anterior liver surfaces abut the diaphragm.
• The left lobe of the liver lies in the left hypochondriac and epigastric regions. It is bounded in front by the rib cage and abdominal wall and posteriorly it rests on the stomach.
• The right lobe occupies the right hypochondrium. It is bounded in front by the rib cage and abdominal wall and posteriorly it rests on the gallbladder, head of the pancreas, right adrenal gland, and right kidney (primarily the superior pole).
• The caudate lobe is located on the posterior surface of the liver and lies posterior to the porta hepatis between the fissure for the ligamentum venosum and the IVC.
Anatomy
• The liver is considered the largest internal organ of the body. Its mass displaces the gas-filled components of the digestive system, providing an acoustic window for viewing upper abdominal and retroperitoneal structures.
• Size and shape are variable. Anteroposterior size is normal up to 15 cm. Viewed anteriorly, it has a basic wedge shape, tapering toward the left side. The right lobe is significantly larger than the left lobe.
• The entire liver is encased by Glisson’s capsule, a thick, fibrous, connective tissue layer that contains nerves, blood vessels, and lymphatic vessels. In turn, the encased liver is largely covered by the peritoneum.
• The liver is divided into lobes according to anatomy and into segments according to function:
Liver Lobes
Using the traditional anatomic system, the liver is divided based on the sonographic identification of specific anatomic landmarks.
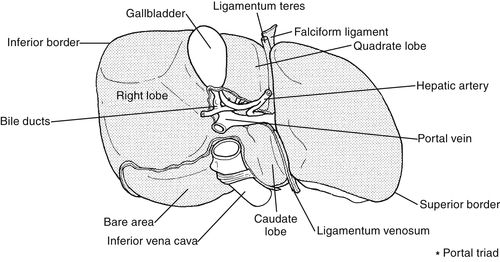
(a) Left lobe: Anatomically separated from the right lobe by the falciform ligament on its superior surface. Divided from the caudate lobe by the fissure for the ligamentum venosum and on its inferior (visceral) surface from the quadrate lobe by the fissure for the ligamentum teres.
(b) Right lobe: Anatomically separated from the left lobe by the falciform ligament on its superior (diaphragmatic) surface and by the left intersegmental fissure on its inferior surface. Riedel’s lobe, a normal anatomic variant, is a projection of the right lobe that can extend as far as the iliac crest.
(c) Caudate lobe: Anatomically separated from the left lobe by the fissure for the ligamentum venosum. Boundaries are the IVC on the right, its margin on the left, which forms the hepatic boundary of the superior recess of the lesser sac, and the porta hepatis anteriorly.
(d) Quadrate lobe: Distinguished sonographically and physiologically as the medial portion of the left lobe. The porta hepatis borders posteriorly, the margin of the liver anteriorly, the gallbladder fossa right laterally, and on the left, the fissure for the ligamentum teres.
Liver Segments
Liver segments are based on hepatic function. Segments are determined according to blood supply and biliary drainage. Segmental liver anatomy is clinically significant for localizing potentially resectable liver lesions.
(a) Two main functional divisions: right and left. Middle hepatic veins located in the main lobar fissure delineate the liver into intrahepatic (functional), right and left lobes:
• The right functional lobe is everything to the right of the plane through the gallbladder fossa and IVC (analogous to the anatomic right lobe).
▪ Two divisions: anterior segment and posterior segment: The right hepatic vein, located in the right intersegmental fissure, delineates the anterior and posterior segments. These segments are also separated by the right portal vein that passes centrally within them.
• The left functional lobe is everything to the left of the plane through the gallbladder fossa and IVC (analogous to the anatomic left lobe, caudate lobe, and quadrate lobe).
▪ Two divisions: medial segment and lateral segment: The medial segment is analogous to the traditional quadrate lobe. The lateral segment is analogous to the anatomic left lobe. The ascending portion of the left portal vein (in the left intersegmental fissure) delineates the medial and lateral segments. These segments are also separated by the left hepatic vein (in the left intersegmental fissure) superiorly and the ligamentum teres inferiorly.
(b) Caudate lobe: the portion of the liver lying posterior to the porta hepatis, between the fissure for the ligamentum venosum and the IVC.
• No divisions: It distinctly receives hepatic arterial and portal venous blood from both the right and left systems, which otherwise individually supply respective right and left lobes. The left portal vein separates the caudate lobe from the medial segment of the left lobe. The left portal vein runs anterior to the caudate and posterior to the medial segment. The fissure for the ligamentum venosum runs along the left anterior margin of the caudate separating it from medial and lateral segments of the functional left lobe.
Liver Surfaces
The different surfaces of the liver include distinctions among the posterior, anterior, superior, and inferior surfaces.
(a) Posterior surface:
• Caudate lobe.
• Bare area.
• Deeply indented area centrally where it lies on the spine.
• Fossae for the IVC and ligamentum venosum.
• Attachment to the diaphragm by loose connective tissue.
• Most of this surface is not covered by peritoneum.
(b) Anterior surface:
• Lies inside the peritoneum immediately posterior to the xiphoid process of the sternum.
• Is part of the diaphragmatic surface until it loses contact on the left at the seventh or eighth costal cartilage and on the right anywhere from the 6th to the 10th costal cartilage.
• Is accentuated by a deep notch. The ligamentum teres ascends from the umbilicus to the umbilical notch of the anterior surface.
(c) Superior surface:
• Is intraperitoneal.
• Is a convex diaphragmatic, smooth surface, separated from the pleura, lungs, pericardium, and heart by the dome of the diaphragm.
(d) Inferior surface:
• Is covered by peritoneum except at the porta hepatis and site of the gallbladder attachment.
• Is a concave visceral surface accentuated by fossae and indentations from organs that rest against its surface.
• Of the left lobe is deeply indented by the anterior surface of the stomach.
• Of the right lobe is accentuated by the hepatic flexure of the colon, right kidney and adrenal gland, and the duodenum, where it lies adjacent to the gallbladder neck.
• Anterior mid portion is the quadrate lobe (medial left lobe) bound by the falciform ligament on the left.
• Posterior mid portion of the inferior surface is the caudate lobe. The posterior portion of the caudate forms a part of the anterior boundary of the lesser sac.
Liver Ligaments
Liver ligaments attach the liver to the diaphragm, stomach, anterior abdominal wall, and retroperitoneum. Liver ligaments are viewable with ultrasound because of the fat and collagen within and around these structures. This makes them quite hyperechoic relative to hepatic parenchyma. The different types of liver ligaments include the falciform ligament, ligamentum teres, coronary ligament, right and left triangular ligaments, gastrohepatic ligament, and hepatoduodenal ligament.
(a) Falciform ligament: Parietal peritoneal, anteroposterior fold that attaches the bare area of the liver to the right rectus muscle of the anterior abdominal wall. It extends from the diaphragm to the umbilicus, running along the liver’s anterior surface. It is continuous with the ligamentum teres, which is contained within its layers. On the liver’s superior (diaphragmatic) surface, it is described as the anatomical divider of the right and left lobes and along with the ligamentum teres, functionally designates the boundary of the left lobe’s medial and lateral segments.
(b) Ligamentum teres: Fibrous, round ligament formed by the obliterated left umbilical vein. Arises from the umbilicus and courses within the falciform ligament to the umbilical notch on the anterior surface of the liver. Coursing along the inferior (visceral) surface, it continues as the ligamentum venosum (obliterated ductus venosus) running posteriorly to the IVC.
(c) Coronary ligament: Parietal peritoneal, bifold layer that attaches the liver’s posterior surface to the diaphragm. Anterior and posterior layers are continuous anteriorly with the falciform ligament and laterally with the triangular ligaments.
(d) Right and left triangular ligaments: Formed by continuations of the coronary ligament. Triangular extensions on the right from the far right border of the bare area to the diaphragm and on the left from the superior surface of the left lobe to just anterior of the esophageal opening in the diaphragm.
(e) Gastrohepatic ligament: Visceral peritoneal, bifold layer also known as the lesser omentum. From the undersurface of the liver, it is continuous with the ligamentum venosum. Ascending, it attaches the undersurface with the lesser curvature of the stomach and the first portion of the duodenum.
(f) Hepatoduodenal ligament: Portion of the lesser omentum that is located on the right free edge of the gastrohepatic ligament. Extends to the duodenum and right hepatic flexure and forms the ventral portion of the foramen of Winslow or the epiploic foramen. Surrounds the portal triad immediately adjacent to the porta hepatis.
Liver Fissures
Liver fissures are the normal grooves or folds throughout the liver that typically form the spaces that contain various blood vessels or ligaments. Ultrasound can identify the fissures associated with the liver due to the fat and collagen within and around them, which makes them highly reflective relative to liver parenchyma. Types of liver fissures include main lobar fissure, left intersegmental fissure, fissure for the ligamentum venosum, and fissure for the ligamentum teres.
(a) Main lobar fissure: Runs obliquely between the neck of the gallbladder and right portal vein. Contains the middle hepatic vein and separates the right and left hepatic lobes. Its course is short and variable.
(b) Left intersegmental fissure: Subdivides the right lobe into anterior and posterior portions.
(c) Ligamentum venosum fissure: Contains the gastrohepatic ligament and separates the left lobe and caudate lobe.
(d) Ligamentum teres fissure: Forms the left boundary of the quadrate or medial portion of the left lobe.
Liver Vessels and Ducts
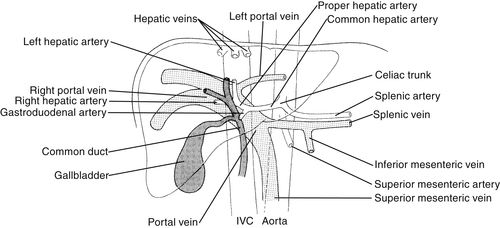
The liver receives nutrient rich blood from the hepatic artery and the portal vein, which is highly saturated with oxygen. The hepatic veins drain the liver of deoxygenated blood. The hepatic ducts transport bile, a fluid made in the liver, to the bile ducts. The bile ducts convey the bile to the gallbladder for storage. When bile is needed to aid digestion of fat, the bile ducts carry it into the duodenum. Structures that make up the liver vessels and ducts include the hepatic arteries, hepatic veins, portal vein, portal venous system, hepatic ducts, and portal triad.
(a) Hepatic arteries: Supply the liver with oxygenated blood from the aorta. The celiac axis branch of the aorta divides into the splenic, left gastric, and common hepatic arteries.
• The proper hepatic artery divides into two main branches, the right and left hepatic arteries which supply the right and left segmental lobes, respectively.
• The middle hepatic artery generally arises from the left hepatic artery.
• The cystic artery arises from the right hepatic artery.
(b) Hepatic veins: The right, middle, and left hepatic veins drain the blood from the liver and empty it into the IVC.
(c) Portal vein: The main portal vein enters the liver at the porta hepatis, posterior to the hepatic artery and common bile duct. It then divides into the right and left branches. These branches become intersegmental veins that branch into medial and lateral portions of the left lobe and anterior and posterior portions of the right lobe.
(d) Portal venous system: Supplies the greatest percentage of total blood flow to the liver. Formed by the confluence of three tributaries:
(1) Splenic vein
(2) Superior mesenteric vein
(3) Inferior mesenteric vein
Commonly referred to as the portal splenic confluence. This system carries blood from the spleen and bowel to the liver.
(e) Hepatic ducts: Enzymatic bile is manufactured in the liver then transferred via the right and left hepatic ducts from the liver to the extrahepatic bile ducts at the porta hepatis. As the right and left hepatic ducts emerge from liver parenchyma at the porta hepatis, they unite to form the common hepatic duct, which courses inferomedially where it is joined by the cystic duct to form the common bile duct. The common bile duct descends to cross behind the first portion of the duodenum to enter into or run along the posterior portion of the parenchyma of the head of the pancreas. From there it courses slightly toward the right and enters the second portion of the duodenum, where it ends at the ampulla of Vater. The extrahepatic bile ducts (common hepatic, cystic, common bile) maintain communication between the liver and gastrointestinal tract.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


