Overview
Location
• The pancreas is retroperitoneal (located in the retroperitoneum, the portion of abdominopelvic cavity posterior to the peritoneal sac). It extends from the second portion of the duodenum, across the midline, to the hilum of the spleen.
• The descriptive portions of the pancreas are located as follows:
(b) Uncinate process: A medial extension of the head that lies directly posterior to the superior mesenteric vein. It has been known to extend as far left as the aorta.
(c) Neck: The portion of pancreas directly anterior to the superior mesenteric vein.
(d) Body: The portion of pancreas that extends left lateral from the neck and lies between the posterior wall of the antrum of the stomach and the superior mesenteric artery. Its left lateral border is generally described as not definite.
(e) Tail: The portion of pancreas that typically lies posterior to the stomach, between the left lateral edge of the spine and the hilum of the spleen.
Anatomy
• The pancreas is a nonencapsulated multilobular gland. Its blood supply is from the superior mesenteric artery, splenic artery, and gastroduodenal artery. Venous drainage is through splenic and superior mesenteric vein tributaries.
• Wirsung’s duct, the main pancreatic duct, extends the length of the pancreas and enlarges toward the head up to 3 mm. It meets with the common bile duct at the pancreas head, and joined together or separately, the ducts enter the second portion of the duodenum.
• Santorini’s duct is a normal variant that serves as an accessory pancreatic duct from the anterior portion of the pancreas head. It enters the duodenum superior to and separate from Wirsung’s duct and the common bile duct.
• The size, shape, and lie of the pancreas vary somewhat. The size decreases with age. The shape has been compared to a dumbbell, sausage, and a comma with the larger segment representing the head. The lie or orientation of the pancreas has varying degrees of horizontal oblique.
• The normal adult pancreas is 15 to 20|cm in length.
• The anterior to posterior dimensions of the head range from 2.0 to 3.0|cm.
• The anterior to posterior dimensions of the neck range from 1.5 to 2.5|cm.
• The anterior to posterior dimensions of the body range from 1.5 to 2.5|cm.
• The anterior to posterior dimensions of the tail range from 1.0 to 2.0|cm.
Physiology
• The pancreas has both endocrine and exocrine functions:
• Endocrine function: produces the hormone insulin to prevent diabetes mellitus.
• Exocrine function: produces pancreatic enzymes that, via the pancreatic ducts, aid digestion.
Sonographic Appearance
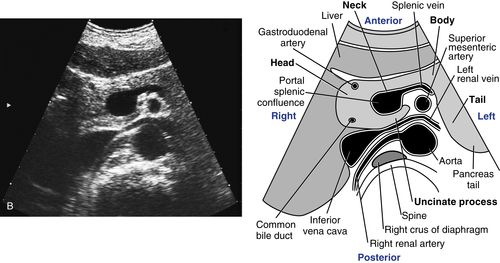
• Because the pancreas lies at a horizontal oblique in the body, the longitudinal and long axis sections are visualized in an obliqued transverse scanning plane. The following obliqued, transverse scanning plane image shows the long axis of a normal adult pancreas.

Notice how the pancreas appears midgray, with even texture that is moderately hyperechoic relative to the normal liver (in many cases the pancreas will appear isosonic to the liver). Observe the smooth contour of the pancreas and how it is distinguishable from adjacent structures (the pancreas is nonencapsulated, so it can be infiltrated by retroperitoneal fat making the contour uneven and difficult to evaluate in some cases). The anechoic, longitudinal section of the splenic vein running along the posterior margin of the pancreas body serves as an easily recognizable vascular landmark when identifying the pancreas. Notice how the splenic vein (coming from the splenic hilum) courses along the posterior aspect of the pancreas to join with the superior mesenteric vein directly behind, or posterior to, the pancreas neck (they join to form the portal vein).
The head of the pancreas is easily identified as it sits directly in front of, or anterior to, the inferior vena cava and is distinguished by the small anechoic axial sections of the gastroduodenal artery on its anterolateral border and the common bile duct on its posterolateral border. The pancreas tail is usually the most difficult part of the pancreas to visualize because it lies behind, or posterior to the stomach; however, it is well demonstrated in this image. Observe how the tail is left lateral to the spine and aorta and more posterior than the pancreas head.
• The axial sections of the pancreas are visualized in sagittal scanning planes (pictured on the facing page). The top scan A, is a sagittal scanning plane image showing an axial section of the pancreas head. It is easily identified as it sits directly anterior to the anechoic, longitudinal inferior vena cava and is distinguished by the small, anechoic, longitudinal sections of the gastroduodenal artery on its anterior border and the common bile duct on its posterior border.

The anatomy in the bottom image B, is the same as the anatomy in the top image but the view is different. Now we see a transverse scanning plane image showing a long section of the pancreas; the head is clearly distinguished as it sits just anterior to the anechoic, axial inferior vena cava and the anechoic, axial sections of the gastroduodenal artery (anteriorly) and the common bile duct (posteriorly) are easily identified.

• The next images demonstrate axial and longitudinal views of the pancreas neck, uncinate process, and the superior mesenteric vein that separates them. The top scan A, is a sagittal scanning plane image, showing a longitudinal view of the superior mesenteric vein separating axial sections of the pancreas neck (seen anteriorly) and uncinate process (seen posteriorly). The bottom image B, is the same as the anatomy in the top image but the view is different. Now we see a transverse scanning plane image showing longitudinal views of the pancreas neck (anteriorly) and uncinate process (posteriorly), clearly separated by the anechoic, round, axial section of the superior mesenteric vein.


• The splenic vein and superior mesenteric artery serve as vascular landmarks when identifying the body of the pancreas. The top scan A, is a sagittal scanning plane image demonstrating an axial view of the pancreas body. Observe how the body is seen directly anterior to the anechoic, axial section of the splenic vein, which lies just anterior to the anechoic superior mesenteric artery seen in longitudinal section as it branches from the aorta. The splenic artery marks the superior edge of the pancreas body. Two anechoic, round, axial sections of the splenic artery are easily identified in this image. The anatomy in the bottom transverse scanning plane image B, is the same as the anatomy in the top image but the view is different. Now we see a longitudinal view of the pancreas body. Notice how the body sits just anterior to an anechoic, long section of the splenic vein, which is just anterior to the anechoic, round, axial section of the superior mesenteric artery.

• The splenic vein also serves as a vascular landmark when identifying the tail of the pancreas. The left kidney is helpful when locating the tail as well (pictured below). The top scan A, is a sagittal scanning plane image, showing an axial section of the pancreas tail seen anterior to the anechoic, long splenic vein section and left kidney. The bottom scan B, is a transverse scanning plane image demonstrating the same anatomy as the top image but the view is different. Now we see a longitudinal view of the pancreas tail clearly anterior to the anechoic, axial splenic vein section, left lateral to the spine and posterior to the stomach. Note the left kidney directly posterior to the splenic vein.


• Wirsung’s duct (or the pancreatic duct) is commonly seen and most frequently in the body portion of the pancreas. It appears anterior to the anechoic, long splenic vein sections either as a long, thin, bright line or as an anechoic, longitudinal section bordered by thin, bright walls as seen in the following image:

Normal Variants
• The size, shape, and lie of the pancreas are normally variable.
• The duct of Santorini is a normal variant accessory duct.
Preparation
Patient Prep
• The patient should fast for 8 to 12 hours before the study. This reduces the amount of stomach and bowel gas anterior to the pancreas and ensures normal gallbladder and biliary tract dilatation, which is significant because the pancreas and biliary tract are interdependent systems.
• If the patient has eaten, still attempt the examination because in some cases, stomach contents can displace gas and serve as a “window” for the sound beam. Also, for this reason, the patient can be given 2 to 4 cups of water or noncarbonated drink to provide a sonic window and displace any gas in the stomach that may be obscuring the view of the pancreas. In most cases, this fluid technique works best if the patient is sitting erect.
Transducer
• Curved array 5.1 MHz or 5.2 MHz.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


