Bronchiectasis is most simply defined as irreversible bronchial dilatation. It is usually associated with structural abnormalities of the bronchial wall, and chronic or recurrent infection is usually present. Bronchiectasis may occur as a result of various pathologic processes and thus may be a feature of a number of different lung and airway diseases (1, 2, 3, 4).
Although chronic cough and expectoration of purulent sputum are common in patients with bronchiectasis, symptoms and physiologic abnormalities are usually nonspecific and a clinical diagnosis is often difficult to make. On the other hand, because bronchiectasis is defined by abnormal morphology, imaging provides an accurate diagnosis in most cases. Volumetric spiral computed tomography (SCT) with thin slices and high-resolution computed tomography (HRCT) are both highly accurate in the diagnosis of bronchiectasis and are routinely used in clinical practice.
PATHOLOGY OF BRONCHIECTASIS
Regardless of its cause, bronchiectasis is usually associated with (a) bronchial wall inflammation and infiltration by inflammatory cells; (b) destruction of the elastic, muscular, and cartilaginous elements of the bronchial wall; (c) bronchial wall fibrosis; (d) irregularity of the bronchial lumen; (e) chronic infection; (f) mucous plugging; and (g) replacement of the ciliated epithelium by squamous or columnar epithelium in some cases. The surrounding lung parenchyma often shows evidence of fibrosis, inflammation, atelectasis, and sometimes pneumonia. Bronchioles often demonstrate abnormalities similar to those affecting the larger airways, and constrictive bronchiolitis (bronchiolitis obliterans) may be present (1, 2, 3, 4).
PATHOGENESIS
Several mechanisms are involved in the development of bronchiectasis. These include bronchial infection, inflammation, peribronchial fibrosis, and bronchial obstruction (Table 4-1). Underlying structural abnormalities of the bronchial wall, either congenital or acquired, may also be present in some patients. In many patients with bronchiectasis, several mechanisms acting in concert contribute to the development of airway abnormalities. Infection is almost always present.
Infection
The most common cause of bronchiectasis is acute, chronic, or recurrent infection. In otherwise healthy individuals, acute infection by organisms capable of causing tissue necrosis may lead to bronchial wall destruction and bronchiectasis. Such infections include tuberculosis (TB), pertussis, staphylococcus, and viral diseases. In such cases, a single childhood illness may result in eventual bronchiectasis.
In other patients, underlying conditions that predispose them to chronic airway infection may lead to bronchiectasis. Such conditions include (a) congenital or acquired immune deficiency and (b) abnormal bronchial mucociliary clearance related to ciliary abnormalities (e.g., dyskinetic cilia syndrome), abnormal mucus (e.g., cystic fibrosis), bronchial obstruction (e.g., neoplasm), or structural bronchial abnormalities (e.g., tracheobronchomegaly) (1,5, 6, 7). In patients with chronic infection, cytokines released by macrophages and airway epithelial cells result in neutrophil recruitment and subsequent release of elastase, collagenase, and other active substances; these lead to airway wall inflammation and destruction. Common organisms found on sputum culture of patients with chronic bronchiectasis include Haemophilus influenzae (29% to 42% of patients), Pseudomonas aeruginosa (13% to 31%), Streptococcus pneumoniae (6% to 13%), Branhamella catarrhalis, and Staphylococcus aureus, in approximate order of frequency (1).
It is crucial to recognize that the presence of bronchial dilatation itself (i.e., bronchiectasis) results in abnormal mucociliary clearance, which in turn predisposes a patient to chronic bronchial infection. To make matters worse, infection may contribute to abnormal mucociliary clearance through release of toxins from the infecting organisms; these may cause abnormalities of ciliary function. In this manner, a vicious circle is created: bronchiectasis and infection lead to abnormal airway clearance, which predisposes the airway to infection, which results in further airway wall inflammation and destruction.
TABLE 4-1 CAUSES OF BRONCHIECTASIS AND POSSIBLE MECHANISMS
Bronchial wall inflammation, epithelial damage, recurrent infection in some cases
Aspiration, toxic fume inhalation
Inflammation
Modified from Davis AL, Salzman SH, eds. Bronchiectasis. Philadelphia: WB Saunders, 1991.
Inflammation
Bronchiectasis may also result from bronchial inflammation without obvious infection in patients with collagen vascular diseases, inflammatory bowel disease, bronchiolitis obliterans, or allergic bronchopulmonary aspergillosis or in those who inhale toxic fumes or aspirate corrosive liquids.
Fibrosis
Peribronchial fibrosis, occurring in conjunction with bronchial and peribronchial infection (i.e., in patients with bronchiectasis) or fibrotic lung disease (e.g., TB, sarcoidosis, usual interstitial pneumonia) may result in or contribute to bronchial dilatation. In patients with bronchiectasis resulting from chronic infection, peribronchial fibrosis undoubtedly contributes to bronchial dilatation and luminal irregularity. In patients with fibrotic lung disease, fibrous tissue results in traction on the bronchial wall and causes them to dilate. Bronchiectasis related to fibrotic lung diseases is termed “traction bronchiectasis” (8). It is not a primary airway disease and is not characteristically associated with airway infection or typical symptoms of bronchiectasis. Traction bronchiectasis is best thought of as a sign of lung fibrosis and not an airway disease.
Bronchial Obstruction
Bronchial narrowing or obstruction with accumulation of mucus distal to the obstruction and chronic infection may lead to bronchiectasis. Bronchial obstruction may occur because of endobronchial neoplasm, foreign body, postinflammatory stricture, or congenital bronchial abnormality (e.g., bronchial atresia) or as a result of external compression.
Structural Bronchial Abnormalities
In patients with bronchiectasis occurring because of other causes, chronic infection and inflammation result in destruction of the elastic, muscular, and cartilaginous elements of the bronchial wall, leading to bronchial dilatation. Uncommonly, bronchiectasis results from an inherent structural abnormality of the bronchial wall that predisposes the bronchi to dilatation. Examples include Williams-Campbell syndrome and tracheobronchomegaly, in which cartilaginous, elastic, or muscular elements of the bronchial wall are deficient.
CLINICAL PRESENTATION
The presentation of patients with bronchiectasis is often nonspecific. In general, a clinical diagnosis of bronchiectasis is possible only in the most severely affected patients, and even in this setting, differentiation from chronic bronchitis or other airway diseases may be difficult (9).
Patients with bronchiectasis may have symptoms related to both airway infection and underlying or associated conditions, such as chronic bronchitis, emphysema, asthma, or bronchiolitis obliterans. Nearly all patients with bronchiectasis have chronic cough with purulent sputum production and recurrent pulmonary infections (1,2,4, 5, 6,10). Other symptoms may include fever, wheezing, chest pain, and weight loss. Hemoptysis also is frequent, occurring in up to 50% of patients, and may be the only clinical finding; it usually reflects the presence of bronchial artery enlargement associated with chronic inflammation (6,11,12).
Pulmonary function test (PFT) findings vary with the underlying cause of the bronchiectasis. However, most patients have some degree of airflow obstruction; mild restriction and hypoxemia also may be present (1,4,13). The presence of obstructive abnormalities on PFTs may partially reflect the collapse of abnormal bronchi with expiration but is more likely related to associated small airway abnormalities, such as bronchiolitis obliterans, infectious bronchiolitis, and asthma or associated emphysema. Mild restrictive abnormalities are sometimes present on PFTs, usually in patients with diseases resulting in lung fibrosis or reduced lung volume. Low diffusing capacity may be present in some patients with bronchiectasis, perhaps resulting from ventilation-perfusion mismatch.
RADIOGRAPHIC FINDINGS
The radiographic manifestations of bronchiectasis have been well described (14). These include (a) a loss of definition of vascular markings in affected lung segments, presumably resulting from peribronchial fibrosis and volume loss, (b) evidence of bronchial wall thickening with “tram tracks,” (c) obvious bronchial dilatation, manifested in severely affected patients by discrete tubular or cystic lesions, and (d) mucus- or fluid-filled bronchi (Fig. 4-1).
It has been suggested that the radiographic diagnosis of bronchiectasis may be made more sensitive and accurate by the use of specific anatomic criteria (15). The most important of these is assessment of bronchial dilatation, either by comparing the diameters of end-on bronchi in normal and abnormal areas of the lung or by the measurement of bronchoarterial ratios.
Although radiographs are abnormal in 80% to 90% of patients with bronchiectasis, findings are often nonspecific and a definitive diagnosis is usually difficult to make except in advanced cases (9). Overall, the correct diagnosis may be made on chest radiographs in only about 40% of patients.
Figure 4-1 Radiographic appearance of bronchiectasis. Chest radiograph in a patient with severe bronchiectasis associated with cystic fibrosis shows tram tracks and ring shadows resulting from dilated and thick-walled bronchi. Ill-defined nodular opacities represent mucous plugs.
BRONCHOGRAPHIC FINDINGS
Bronchography is rarely used in clinical practice to diagnose bronchiectasis. Nonetheless, the bronchographic findings of patients with bronchiectasis have been described in detail, and knowledge of the typical bronchographic findings is helpful in understanding CT diagnosis of this disease.
Bronchographic findings indicative of bronchiectasis include (a) proximal and/or distal bronchial dilatation, (b) lack of normal tapering of peripheral airways (i.e., cylindrical bronchiectasis), (c) bronchial contour abnormalities (i.e., varicose and cystic bronchiectasis), (d) pruning (reduction in the number) of bronchial branches, (e) luminal occlusion, and (f) luminal filling defects resulting from mucoid or purulent secretions.
CT FINDINGS OF BRONCHIECTASIS
Direct findings of bronchiectasis include bronchial dilatation, bronchial contour abnormalities, lack of normal bronchial tapering, and visibility of airways in the lung periphery (Table 4-2) (2, 3, 4,16,17). Indirect findings of bronchiectasis (i.e., those not directly related to bronchial dilatation) include bronchial wall thickening and irregularity and mucoid impaction of the bronchial lumen. Small airway abnormalities are also often associated with bronchiectasis, with HRCT showing bronchiolectasis, centrilobular nodules, and “tree-in-bud.” A combination of these findings enables an accurate diagnosis in a large percentage of patients.
TABLE 4-2 HRCT FINDINGS IN BRONCHIECTASIS
DIRECT SIGNS
INDIRECT SIGNS
Bronchial dilatation
Increased bronchoarterial ratio Signet-ring sign (vertically oriented bronchi)
Contour abnormalities Cylindrical, varicose, or cystic bronchiectasis
Lack of tapering >2 cm distal to bifurcation
Visibility of peripheral airways within 1 cm of the costal pleura
Bronchial wall thickening
>0.5 times the diameter of an adjacent pulmonary artery (vertically oriented bronchi)
Mucoid impaction or fluid-filled bronchi
Tubular or Y-shaped structures
Branching or rounded opacities in cross section
Air-fluid levels
Centrilobular nodules or tree-in-bud
Mosaic perfusion
Air trapping on expiratory scan
Bronchial artery hypertrophy
Atelectasis or emphysema
Additional CT findings that may be seen in some patients with bronchiectasis include mosaic perfusion visible on inspiratory scans, focal air trapping identifiable on expiration scans, tracheomegaly, bronchial artery enlargement, atelectasis, and emphysema.
Bronchial Dilatation
Because bronchiectasis is defined by the presence of bronchial dilatation, recognition of increased bronchial diameter is key to the CT diagnosis of this abnormality. Various methods for measuring airway dimensions have been proposed. These include the use of digital image analysis programs requiring operator-dependent definition of a “seed point” at the lumen-wall interface to obtain isocontour lines of the bronchial lumen (18) and automated thresholding to detect the airway lumen area (19). Although these approaches may allow precise quantitative assessment of airways, and may prove particularly valuable in physiologic studies, subjective visual criteria for establishing the presence of bronchial dilatation are most often used in the interpretation of clinical scans (20, 21, 22, 23, 24, 25).
For the purposes of CT interpretation, bronchial dilatation may be diagnosed (a) by comparing the bronchial diameter to that of the adjacent pulmonary artery branch (i.e., determining the bronchoarterial ratio), (b) by detecting a lack of bronchial tapering, and (c) by identifying airways in the peripheral lung.
Bronchoarterial Ratio
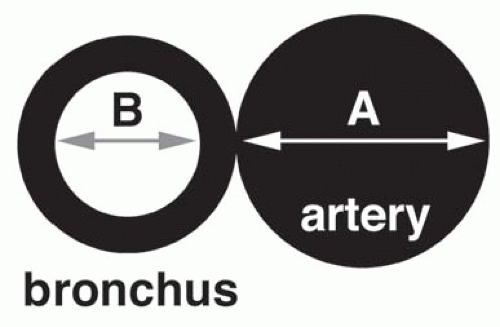
In most normal subjects, the diameters of bronchi and adjacent pulmonary arteries are nearly the same. Their diameters may be compared by using the bronchoarterial ratio (B/A ratio), defined as the internal diameter (i.e., luminal diameter) of the bronchus divided by the diameter of the adjacent pulmonary artery (Fig. 4-2). To avoid the exaggeration of diameters caused by obliquity of the bronchus and artery relative to the scan plane, the least diameter of the bronchus and artery are used for measurement. The B/A ratio in normal subjects generally averages 0.65 to 0.70 (Fig. 4-3) (26,27).
The definition of an abnormal or increased B/A ratio varies widely among authors (16,20,22,24,25,27,28). In most cases, bronchiectasis is considered to be present when the internal diameter of a bronchus is greater than the diameter of the adjacent pulmonary artery branch, that is, when the B/A ratio is greater than 1 (16). The accuracy of this finding in diagnosing bronchiectasis has been validated in a number of studies comparing CT with bronchography in patients with bronchiectasis (29, 30, 31, 32). A B/A ratio of more than 1 is recognizable on HRCT in 95% of patients with bronchiectasis (21).
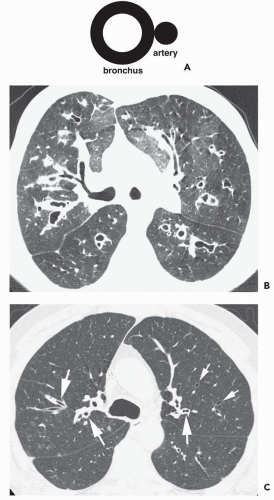
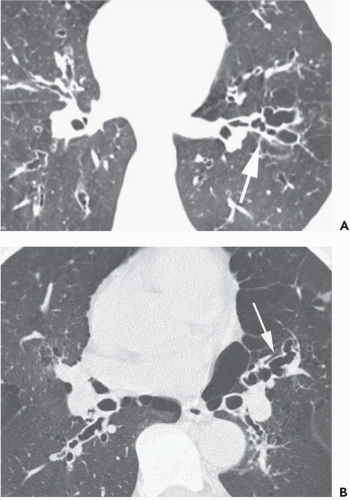
However, in patients with bronchiectasis, the bronchial diameter is often much larger than the pulmonary artery diameter (i.e., the B/A ratio is >1.5), a finding that reflects not only the presence of bronchial dilatation but also some reduction in pulmonary artery size as a consequence of decreased lung perfusion in affected lung regions (i.e., mosaic perfusion) (21). The association of a dilated bronchus with a much smaller adjacent pulmonary artery branch has been termed the signet-ring sign (Fig. 4-4) (33). This classic sign is very useful in recognizing bronchiectasis and in distinguishing dilated airways from other cystic lung diseases, which tend not to be associated with this finding.
Figure 4-2 Bronchoarterial ratio (B/A ratio). The B/A ratio is calculated by dividing the internal diameter (i.e., luminal diameter) of the bronchus (B) by the diameter of the adjacent pulmonary artery (A).
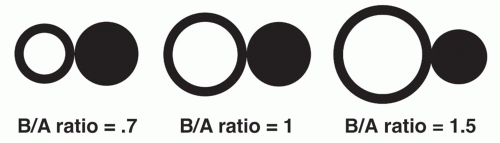
Figure 4-3 Normal and abnormal bronchoarterial (B/A) ratios. A normal B/A ratio averages 0.65 to 0.7 in young or middle-aged patients. A B/A ratio of 1 or more may be seen in some normals older than 65 years or in patients living at high altitude. A B/A ratio of 1.5 is typical of bronchiectasis and usually reflects increased bronchial diameter and decrease in size of the artery. This appearance mimics a signet ring and is termed the signet-ring sign.
Although an abnormal B/A ratio is typical of bronchiectasis, a B/A ratio slightly exceeding 1 may be seen in some normal subjects. For example, in an HRCT evaluation of 14 normal subjects (27), although the B/A ratio averaged 0.65 ± 0.16, 7% of scan interpretations were felt to show some evidence of bronchial dilatation.
The presence of a B/A ratio >1 in normal subjects has been associated with increasing age. In a study by Matsuoka et al. (26), B/A ratios were measured at the segmental and subsegmental levels in the apical and posterior basal segments in 85 normal subjects. A significant correlation was found between the B/A ratio and age (r = 0.768, p <.0001). When the subjects were considered in three age groups, the mean B/A ratios were 0.609 ± 0.05 in subjects 21 to 40 years old, 0.699 ± 0.067 in subjects 41 to 64 years old, and 0.782 ± 0.078 in subjects 65 years and older (p <.0001). At least one bronchus with a B/A ratio >1 was seen in 41% of patients older than 65 years, and in this group, 19% of measured bronchi had a B/A ratio >1. Seven percent of subjects 41 to 64 years of age had at least one bronchus (5% of measured bronchi) with a B/A ratio greater than 1. None of the subjects 21 to 40 years of age showed this finding.
An increase in normal B/A ratio may also be seen in subjects living at high altitude (21,23,24). It has been suggested that this results from mild hypoxemia with bronchial dilatation and vasoconstriction; the same mechanism may result in an increased B/A ratio in older patients. Kim et al. (21) found that 9 (53%) of 17 normal subjects living at an altitude of 1,600 meters had evidence of at least one bronchus equal to or greater in diameter than the adjacent pulmonary artery; these authors found that only 2 of 16 (12.5%) individuals living at sea level similarly showed a similar finding. In this study, the mean B/A ratio was 0.76 at an altitude of 1,600 meters, greater than that seen in subjects living at sea level. Similarly, Lynch et al. (23) compared the internal diameters of lobar, segmental, subsegmental, and smaller bronchi with those of adjacent pulmonary artery branches in 27 normal subjects living in Denver at an altitude of about 1 mile. The authors found that 37 (26%) of 142 bronchi evaluated, and 59% of individuals, had increased B/A ratios.
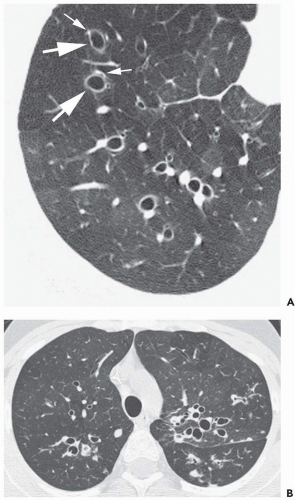
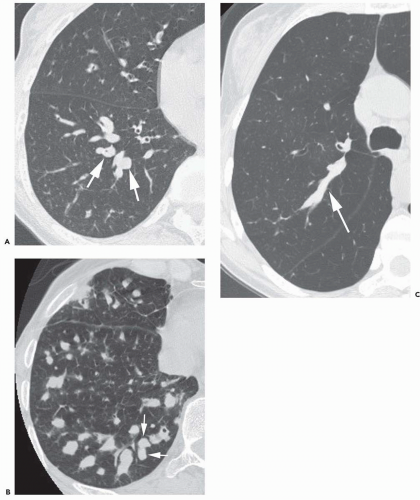
Figure 4-4 Bronchiectasis in two patients with increased B/A ratio. A: Bronchiectasis is visible in the right lower lobe, with increase in the B/A ratio. This is the result of both increase in bronchial diameter (large arrows) and a decrease in size of the accompanying artery (small arrows). This appearance is termed the signet-ring sign. B: Increased B/A ratio in a patient with bilateral upper lobe bronchiectasis. This finding is easiest to recognize when the bronchus and artery are imaged in cross section.
A convincing relationship has not been shown between the B/A ratio and the location of the bronchi being evaluated. Evaluation of the distribution of bronchi with a B/A ratio >1 has generally failed to reveal any relationship to lobe or anteroposterior location within the lungs (21,25).
It must be emphasized that bronchiectasis should not be diagnosed on the basis of an increased B/A ratio alone, unless the B/A ratio is significantly greater than 1 (e.g., 1.5). Bronchial wall thickening is almost always seen in association with bronchial dilatation in patients with bronchiectasis, as are irregularities in bronchial diameter or lack of bronchial tapering. In the normal subjects studied by Lynch et al. (23) who demonstrated an increased B/A ratio, bronchial wall thickening was relatively uncommon, and it is unlikely that any of the subjects in this study would have been diagnosed on clinical HRCT studies as having true bronchiectasis.
Bronchial diameter may be reliably measured using CT, and although objective measurements may be valuable in some cases, visual inspection with a subjective determination of B/A ratio usually suffices for clinical diagnosis (22,34,35). Desai et al. (34) evaluated both interobserver and intraobserver variability in CT measurements of bronchial wall circumference in 61 subsegmental bronchi and found the reproducibility of these measurements to be sufficient for clinical usefulness. Using visual inspection only, Diederich et al. (22) found close agreement among three readers in both the detection (κ = 0.78) and assessment of the severity (κ = 0.68) of bronchiectasis. It should also be pointed out, however, that visual inspection alone may lead to an overestimation of B/A ratio because of an optical illusion in which the diameter of empty circles appears larger than that of solid circles despite their being identical in diameter (21).
A potential limitation of the use of B/A ratios is the necessity of identifying both airways and accompanying arteries. This may not always be possible in patients with coexisting parenchymal consolidation (24). Kang et al. (24), in a study of 47 resected lobes with documented bronchiectasis, were unable to determine the B/A ratios in three patients owing to the presence of parenchymal consolidation.
Lack of Bronchial Tapering
Lack of bronchial tapering has come to be recognized as an important finding in the diagnosis of bronchiectasis and, in particular, subtle cylindrical bronchiectasis. It has been suggested that, for this finding to be present, the diameter of the airway should remain unchanged for at least 2 cm distal to a branching point (Fig. 4-5) (21). First emphasized by Lynch et al. (23) as a necessary finding for diagnosis, lack of bronchial tapering has been reported by some to be the most sensitive means for diagnosing bronchiectasis. Kang et al. (24), for example, in an assessment of 47 lobes with pathologically proved bronchiectasis found lack of tapering of bronchial lumina in 37 cases (79%) as compared with increased B/A ratios seen in only 28 (60%). In another study (36), lack of tapering of bronchi was seen in 10% of HRCT interpretations in healthy subjects compared with 95% of reviews in patients with bronchiectasis. It should be emphasized that the accurate detection of this finding is difficult in the absence of contiguous HRCT sections or thin-collimation SCT, especially for vertically or obliquely oriented airways. The value of this sign is doubtful when HRCT scans are obtained in spaced intervals in a noncontiguous fashion.
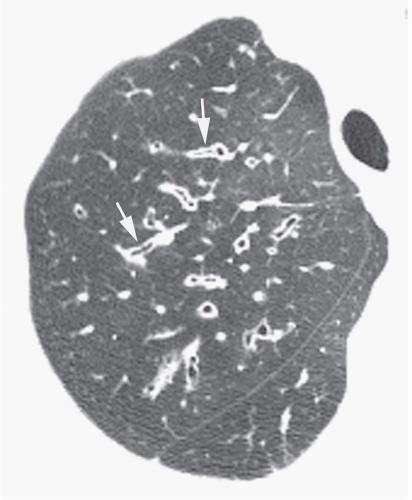
Figure 4-5 Lack of bronchial tapering in bronchiectasis. Two upper lobe bronchi (arrows) show a lack of bronchial tapering distal to a branch point. This is easiest to recognize when the bronchi lie in the plane of the scan.
Visibility of Peripheral Airways
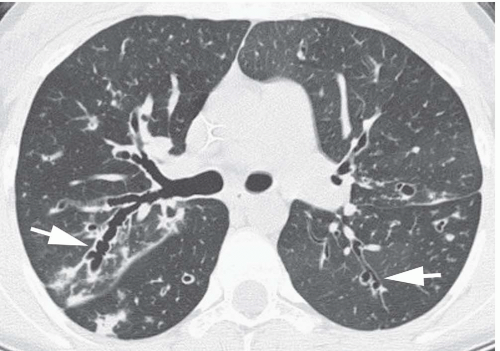
Another finding valuable in the diagnosis of bronchiectasis is visibility of airways in the peripheral 1 cm of lung (Fig. 4-6) (24,36). The smallest airways normally visible using HRCT or thin-collimation SCT techniques have a diameter of approximately 2 mm and a wall thickness of about 0.2 to 0.3 mm (37); in normal subjects, airways in the peripheral 2 cm of lung are uncommonly seen because their walls are too thin (38).
Peribronchial fibrosis and bronchial wall thickening in patients with bronchiectasis, in combination with dilatation of the bronchial lumen, allow small airways in the lung periphery to be seen on HRCT or thin-slice SCT. In a study by Kang et al. (24), bronchi visualized within 1 cm of pleura were seen in 21 of 47 (45%) bronchiectatic lobes.
Kim et al. (36) further assessed the value of this sign in the diagnosis of bronchiectasis. The authors emphasized that although normal bronchi are not visible within 1 cm of the costal pleural surfaces, they may be seen within 1 cm of the mediastinal pleural surfaces. In their study, bronchi were visible within 1 cm of the mediastinal pleura in 40% of normal subjects (36). Bronchi within 1 cm of the costal pleural surface or bronchi touching the mediastinal pleural surfaces were visible in 81% and 53%, respectively, of HRCT interpretations in patients with clinical or pathologic evidence of cylindrical bronchiectasis.
Bronchial Wall Thickening
Although bronchial wall thickening is a nonspecific finding seen in various airway diseases, it is usually present in patients with bronchiectasis (Fig. 4-6).
Anatomically, the normal thickness of an airway wall is related to its diameter. Second- to fourth-generation (lobar to segmental) bronchi have a wall thickness of approximately 1.5 mm and a mean diameter between 5 and 8 mm (i.e., the bronchial wall thickness is about 20% to 30% of the bronchial diameter), sixth- to eighth-generation (subsegmental) airways have a wall approximately 0.3 mm thick and a mean diameter between 1.5 and 3 mm (the airway wall is 10% to 20% of its diameter), and eleventh- to thirteenth-generation airways have a diameter measuring 0.7 to 1 mm with walls of 0.1 to 0.15 mm (the airway wall is about 15% of its diameter) (39,40).
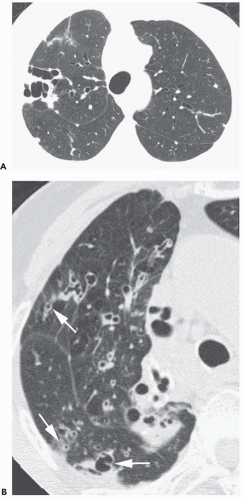
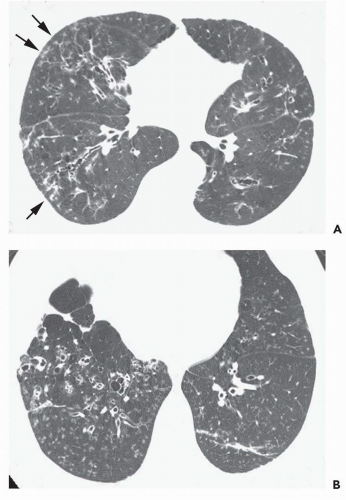
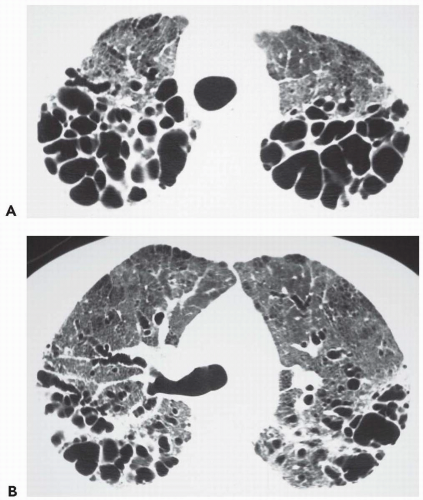
Figure 4-6 Visible bronchi in the peripheral 1 cm of lung in two patients with bronchiectasis. A: Dilated bronchi are seen extending to the pleural surface in the right upper lobe. The bronchial walls are abnormally thickened, and the bronchi are markedly dilated (i.e., cystic bronchiectasis). B: Dilated bronchi are visible about 1 cm from the pleural surface.
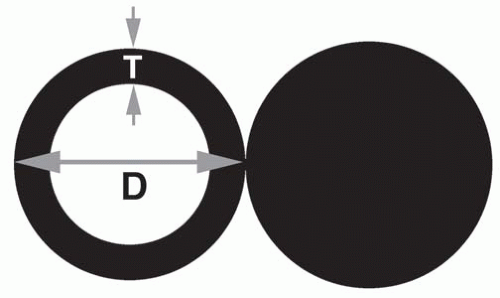
This relationship between bronchial wall thickness and diameter may be expressed by using the thickness-to-diameter (T/D) ratio, defined as wall thickness (T) divided by the total diameter of the bronchus (D) (Fig. 4-7). This ratio may be measured using CT and averages about 20% for segmental and subsegmental bronchi, similar to the anatomic measurements described previously. In one study (26), HRCT was performed in 85 subjects without cardiopulmonary disease. The T/D ratio was measured at the segmental and subsegmental levels of the apical and posterior basal segments. The images were viewed at a window level of −450 H and a window width of 1500 H, thought best for accurate bronchial measurements (41,42). Overall, the T/D ratio measured 0.200 ± 0.015 (range 0.171 to 0.227). No significant correlation was seen between the T/D ratio and age. Although no significant differences in T/D ratio were seen between smokers and nonsmokers in the entire group studies, the T/D ratio was found to be significantly higher in smokers than in nonsmokers when patients 65 years or older were considered as a separate group (p = .021). In another study, the T/D ratio measured 0.23 (±0.04) in 14 normal subjects (43).
The relationship between bronchial wall thickness and bronchial diameter may also be assessed by using the bronchial lumen ratio (BLR), defined as the inner diameter of the bronchus divided by its outer diameter (25). In essence, the BLR represents 1 − (2 × T/D). At the subsegmental level, the BLR in normal subjects averaged 0.66 ± 0.06, with a range of 0.51 to 0.86 (25).
There is no widespread agreement as to what constitutes bronchial wall thickening or how it should be measured using CT, although various methods have been proposed (22,26,28,44,45). Identification of thickened bronchial walls for the purpose of interpretation of clinical scans remains largely subjective (24,46).
Simply determining the T/D ratio or BLR is problematic in the diagnosis of bronchial wall thickening, because bronchiectasis increases the bronchial diameter at the same time the wall becomes thick (Fig. 4-8A). Comparing the bronchial wall thickness with the diameter of the adjacent pulmonary artery is useful as an objective measurement, and bronchial wall thickening is diagnosed if the airway wall is at least 0.5 times the width of an adjacent vertically oriented pulmonary artery (Fig. 4-8A and B) (28,44,47).
Figure 4-7 Measurement of bronchial wall thickness using the T/D ratio. This ratio is defined as wall thickness (T) divided by the total diameter of the bronchus (D). In normals, it averages about 0.2 or 20%.
Because bronchiectasis and bronchial wall thickening are often multifocal rather than diffuse and uniform, a comparison of bronchi in one lung region with those in another can be helpful in making this diagnosis (Fig. 4-8C). Remy-Jardin et al. (45) considered bronchial wall thickening to be present if a bronchial wall measured twice the thickness of the wall of a similar but normal bronchus.
The quantitative measurement of bronchial wall thickness is tedious and uncommonly performed in clinical practice. Fortunately, it has been shown that visual assessment of wall thickening may be reliable. Using visual estimation, Diederich et al. (22) found acceptable levels of agreement among three readers regarding the presence or absence of bronchial wall thickening (κ = 0.64), although the validity of this diagnosis was not assessed. On the other hand, Bankier et al. (48) found relatively low sensitivity in the diagnosis of abnormally thick-walled segmental and subsegmental bronchi, evaluated by three independent observers, on two occasions. Sensitivity in detecting abnormal bronchi averaged 45% with a specificity of 72% (48), although it should be emphasized that the airway abnormalities evaluated in this study were subtle with abnormal segmental and subsegmental wall thickness measuring 1.77 mm and 0.95 mm, respectively, as compared with normal segmental and subsegmental airways measuring 1.14 and 0.46 mm, respectively.
Mucoid Impaction
The presence of mucus- or fluid-filled bronchi may be helpful in confirming a diagnosis of bronchiectasis. The HRCT appearance of fluid or mucus-filled airways is dependent on both their size and orientation relative to the scan plane (Fig. 4-9). Larger mucus-filled airways result in abnormal lobular or branching structures when they lie in the same plane as the CT scan. Although they may be confused with abnormally dilated vessels, in most cases the recognition of dilated, fluid-filled airways is simplified by the identification of other areas of bronchiectasis in which the bronchi are air filled; these are usually revealed with careful examination. In problematic cases, distinction between larger fluid-filled bronchi and dilated blood vessels is easily made by rescanning patients following the bolus injection of intravenous contrast agent. Alternatively, with the introduction of newer generation scanners, it is possible to obtain high-quality multiplanar and maximum-intensity projection images in a variety of imaging planes as a means for further evaluation.
Although commonly associated with bronchiectasis and infection, dilated mucus-filled airways in the central lung can also result from congenital bronchial abnormalities, such as bronchopulmonary sequestration or bronchial atresia (49, 50, 51, 52, 53, 54). It should also be emphasized that the presence of dilated mucus-filled airways, especially when central or predominantly segmental or lobar in distribution, should alert one to the possibility of central endobronchial obstruction, resulting from either tumor or foreign body aspiration.
Figure 4-8 Increased wall thickness in bronchiectasis. A: Diagram of bronchial wall thickening in bronchiectasis. The bronchus is thick walled, but the T/D ratio is normal (i.e., about 0.2) because the bronchus is dilated. Note that the bronchial wall is more than half the diameter of the adjacent artery. This finding may be valuable in the diagnosis of wall thickening in the presence of bronchiectasis. B: Bronchial wall thickening in bronchiectasis as a result of CF. C: Bronchial wall thickening in bronchiectasis may not be uniform, and thick-walled bronchi (large arrows) can be contrasted with normal bronchi seen in other locations (small arrows).
Small Airway Abnormalities
Most patients with bronchiectasis also have pathologic or HRCT evidence of small airway disease or bronchiolitis (Figs. 4-10 and 4-11). For example, Kang et al. (24) found pathologic evidence of bronchiolitis in 85% of 47 resected lobes in patients with bronchiectasis. These included 18 lobes with inflammatory or suppurative bronchiolitis, 16 lobes with both inflammatory and obliterative bronchiolitis, and 6 lobes with obliterative bronchiolitis. HRCT findings consistent with bronchiolitis were identified in 30 (75%) of the 47 lobes, including a pattern of mosaic perfusion (n = 21), bronchiolectasis (n = 17), and centrilobular nodular and/or branching opacities (i.e., tree-in-bud) (n = 10) (24).
Figure 4-9 Mucous plugging in three patients with bronchiectasis. A: Dilated lower lobe bronchi (arrows) in a patient with postinfectious bronchiectasis are filled with mucus and imaged in cross section. B: Extensive mucous plugging in the right lower lobe in a patient with chronic bacterial infection. Arteries and mucus-filled bronchi are seen adjacent to each other as paired rounded opacities (arrows).C: Posterior segmental bronchus in the right upper lobe is dilated and impacted with mucus in a patient with Mycobacterium avium infection.
Bronchiolitis in patients with bronchiectasis may be recognized on HRCT by the presence of (a) bronchiolectasis (dilatation of small peripheral or centrilobular airways), (b) tree-in-bud (dilatation and mucoid impaction of centrilobular bronchioles), (c) centrilobular nodules, or (d) mosaic perfusion and air trapping. The HRCT findings of bronchiolitis are also described in Chapter 5.
Bronchiolectasis, Tree-in-bud, and Centrilobular Nodules
Dilated air-filled bronchioles may be recognized on HRCT in a centrilobular location in some patients with bronchiectasis, but more often the finding termed tree-in-bud is visible.
Tree-in-bud is very important in the diagnosis of infectious or cellular bronchiolitis and reflects the presence of dilated centrilobular bronchioles, their lumina impacted with mucus, fluid, or pus and often associated with peribronchiolar inflammation (Fig. 4-10) (55, 56, 57, 58, 59). On HRCT, the finding of tree-in-bud is usually easy to recognize. It may be associated with a typical centrilobular branching appearance, with the most peripheral branches being several millimeters from the pleural surface. Abnormal bronchioles that produce a tree-in-bud pattern can usually be distinguished from normal centrilobular vessels by their more irregular appearance, a lack of tapering, and a knobby or bulbous appearance at the tips of small branches. Normal centrilobular arteries are considerably thinner than the branching bronchioles seen in patients with this finding and are much less conspicuous. Furthermore, because tree-in-bud is often patchy in distribution, it is easy to contrast its appearance with that of adjacent normal lung regions.
Tree-in-bud is commonly associated with bronchiectasis. In a study by Aquino et al. (56), 26 of 27 (96%) patients showing tree-in-bud on HRCT also showed bronchiectasis or bronchial wall thickening on HRCT. Furthermore, 25% of patients with bronchiectasis and 18% of patients with infectious bronchitis reviewed in this study showed tree-in-bud, but this finding was not visible in patients with other diseases involving the airways, such as respiratory bronchiolitis, bronchiolitis obliterans, bronchiolitis obliterans organizing pneumonia, and hypersensitivity pneumonitis (56).
Ill-defined centrilobular nodules representing areas of peribronchiolar inflammation or bronchopneumonia may also be seen in patients with bronchiectasis and airway disease (58). They may be associated with bronchiolectasis or tree-in-bud and are commonly present in patients with bronchiectasis associated with active infection.
Figure 4-10 Small-airway abnormalities in bronchiectasis with tree-in-bud. A: In a patient with CF, branching opacities in the lung periphery are typical of tree-in-bud (arrows) and represent small airways impacted by pus. Central bronchiectasis is also visible. B: Extensive tree-in-bud in the right lower lobe in a patient with bronchiectasis and small-airway infection.
Mosaic Perfusion and Air Trapping
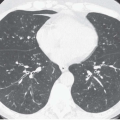
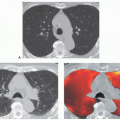
HRCT findings of mosaic perfusion on inspiratory scans and focal air trapping on expiratory scans are useful in the diagnosis of bronchiolitis associated with bronchiectasis (Fig. 4-11). In a study of 70 patients with HRCT evidence of bronchiectasis in 52% of lobes evaluated, areas of decreased attenuation (i.e., mosaic perfusion) were visible on inspiratory scans in 20% of lobes and on expiration (air trapping) in 34% (60). Although areas of decreased attenuation on expiratory scans were more prevalent in lobes with severe bronchiectasis (59% of cases) or localized bronchiectasis (28% of cases), air trapping was identified in the absence of associated bronchiectasis in 17% of lobes. In this same study, the presence of decreased attenuation on expiratory scans was also associated with mucoid impaction. Air trapping was seen in 73% of lobes with large mucus plugs and in 58% of those with centrilobular mucus plugs. These same authors noted a correlation (r = 0.40, p <.001) between the total extent and severity of bronchiectasis and the extent of decreased attenuation shown on expiratory CT. Furthermore, in the 55 patients who had pulmonary function tests, the extent of expiratory attenuation abnormalities was inversely related to measures of airway obstruction such as forced expiratory volume in 1 second (FEV1) and FEV1/forced vital capacity (FVC) (60).
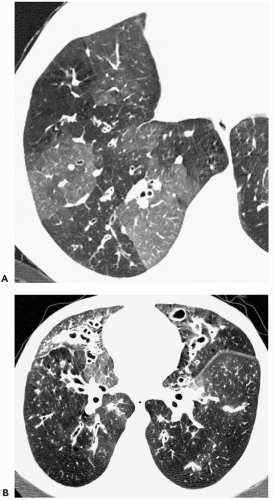
Figure 4-11 Small airway abnormalities in bronchiectasis with mosaic perfusion. A: Patchy mosaic perfusion in CF. Geographic regions of decreased lung attenuation in the right lower lobe are the result of small airway obstruction, poor ventilation, and reflex vasoconstriction. Lucent lung regions contain smaller vessels than dense lung regions. This is diagnostic of mosaic perfusion. Bronchial wall thickening is also visible. B: Mosaic perfusion in CF. Extensive bronchiectasis is visible. Heterogeneous lung attenuation results from mosaic perfusion.
Bronchial Artery Hypertrophy
Bronchial arteries extend from the hila, along the central airways, to a level a few bronchial generations proximal to the terminal bronchioles; they represent the primary bronchial blood supply (61). Arising directly from the proximal descending thoracic aorta, these typically measure <2 mm in size. Enlarged bronchial arteries are identified pathologically in most cases of bronchiectasis, accounting for the common occurrence of hemoptysis in these patients. With thin-slice SCT obtained during contrast infusion, it has proved possible to identify both normal and abnormal bronchial arteries; this is more difficult to do with unenhanced HRCT (62,63).
Song et al. (64) were able to demonstrate good correlation between non-contrast-enhanced HRCT images and corresponding CT angiograms for demonstrating hypertrophied bronchial arteries in patients with bronchiectasis. Specifically, these authors showed that the finding of tubular or nodular areas of soft tissue attenuation, distinct from blood vessels within the mediastinum and adjacent to the central airways, correctly predicted bronchial artery hypertrophy in 88% and 53% of patients, respectively. Although the diagnosis of bronchiectasis rarely is dependent on demonstrating bronchial artery hypertrophy, identification of focal bronchial wall abnormalities resulting from enlarged bronchial arteries is important before attempting bronchoscopy because inadvertent biopsy may lead to significant hemorrhage (64).
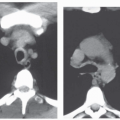
In patients with bronchiectasis and massive hemorrhage, CT can be valuable in determining the cause and localizing the site of bleeding (Fig. 4-12). In a comparison of CT to bronchoscopy in patients with massive hemoptysis, most of whom had bronchiectasis (65), CT was more accurate in identifying the cause of bleeding (77% vs. 8%, respectively; p <.001), whereas the two methods were comparable for identifying the site of bleeding (70% vs. 73%, respectively).
MORPHOLOGIC CLASSIFICATION OF BRONCHIECTASIS
Bronchiectasis traditionally has been classified into three types based on the severity of bronchial dilatation and the degree of luminal irregularity. These three types are cylindrical, varicose, and cystic (66). Although a distinction among these three types of bronchiectasis is sometimes helpful in diagnosis and correlates with the severity of both the anatomic and functional abnormality (28), their differentiation is generally less important clinically than a determination of the extent and distribution of the airway disease.
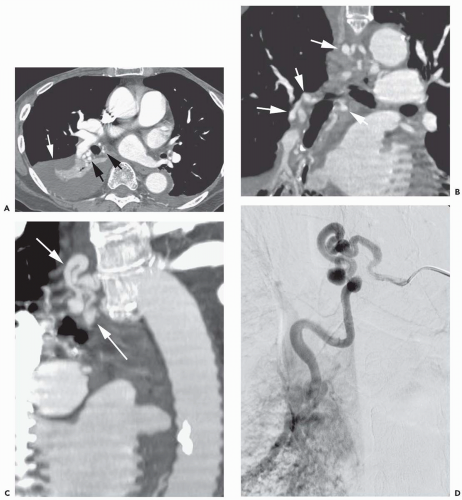
Figure 4-12 Bronchial artery enlargement in bronchiectasis. A: Multidetector CT (1.25-mm slice thickness) during contrast infusion in a patient with hemoptysis. Right lower lobe collapse and consolidation (white arrow) is the result of bronchiectasis. There is marked enlargement of bronchial arteries in the hilum (black arrows).B: Reconstruction in the coronal plane shows enlargement of bronchial arteries in the hilum and mediastinum (arrows).C: Oblique reconstruction shows the enlarged mediastinal bronchial artery (arrows).D: Arteriogram in the same plane as (C) shows bronchial artery enlargement. The bronchial artery was embolized for treatment of the patient’s hemoptysis.
Cylindrical Bronchiectasis
Mild, or cylindrical, bronchiectasis is diagnosed if the dilated bronchi are of relatively uniform caliber and have roughly parallel walls (Fig. 4-13). The appearance of cylindrical bronchiectasis varies depending on whether the abnormal bronchi have a horizontal or a vertical course relative to the scan plane. When horizontal, bronchi are visualized along their length and are recognizable as branching “tram tracks” that fail to taper as they extend peripherally and are visible more peripherally than is normal. When cylindrically dilated bronchi are oriented vertically, they are scanned in cross section and appear as thick-walled, circular lucencies. In most cases, dilated bronchi seen in cross section can be easily distinguished from emphysema or other causes of lung cysts by identifying the signet-ring sign and the continuity of the dilated bronchus on adjacent scans.
Varicose Bronchiectasis
With increasingly severe abnormalities of the bronchial wall, bronchi may assume a beaded configuration, referred to as varicose bronchiectasis (Fig. 4-14). This diagnosis may be difficult to make unless the involved bronchi course horizontally in the plane of the scan. Varicose bronchiectasis is much less frequent than cylindrical bronchiectasis.
Figure 4-13 Cylindrical bronchiectasis in CF. Bronchi are mildly dilated and thick walled. Bronchi seen along their axis have roughly parallel walls (arrows). Bronchi in cross section show the signet-ring sign.
Cystic Bronchiectasis
With severe, or cystic, bronchiectasis, involved airways are cystic or saccular in appearance and may extend to the pleural surface (Fig. 4-15). On HRCT, cystic bronchiectasis may be associated with the presence of (a) air-fluid levels, caused by retained secretions in the dependent portions of the dilated bronchi; (b) a string of cysts, caused by sectioning irregularly dilated bronchi along their length; or (c) a cluster of cysts, caused by multiple dilated bronchi lying adjacent to each other. Clusters of cysts are most frequently seen in atelectatic lobes, presumably as a result of chronic infection.
In general, the dilated airways in patients with cystic bronchiectasis are thick walled, but thin-walled cystic bronchiectasis may be seen in some cases. Recognition of some combination of dilated bronchi, air-fluid levels, and strings or clusters of cysts should be considered diagnostic of cystic bronchiectasis (67).
Figure 4-14 Varicose bronchiectasis in ABPA. A and B: Irregular bronchial dilatation (arrow) is visible.
Figure 4-15 Cystic bronchiectasis. A and B: Cystic lucencies in both upper lobes represent bronchiectasis. Several dilated bronchi have a branching appearance.
Cystic bronchiectasis may be associated with a greater incidence of infection and greater functional impairment than milder forms of disease. In a study of patients with symptomatic bronchiectasis shown on CT (13), patients with cystic bronchiectasis were significantly more likely to grow Pseudomonas from their sputum and to have purulent sputum than were patients with cylindrical or varicose bronchiectasis. Also, patients with cystic bronchiectasis had significantly lower FEV1 and FVC values than did patients with cylindrical or varicose bronchiectasis (13).
ACCURACY OF CT FOR THE DIAGNOSIS OF BRONCHIECTASIS
In our experience, most patients studied using HRCT have clinically suspected disease and subtle abnormalities identified on chest radiographs. Symptomatic patients with entirely normal radiographs are the exception. In a prospective study comparing chest radiographs and HRCT (68), a normal chest radiograph was found to exclude significant bronchiectasis with a high degree of accuracy. In this study, 37 patients had a normal radiograph, and 32 of these had a normal HRCT. The other 5 had mild cylindrical bronchiectasis. In the 47 patients with an abnormal radiograph, 36 had signs of bronchiectasis at HRCT and 11 had a normal HRCT. Thus, in this study, the sensitivity of chest radiography for detecting bronchiectasis diagnosed by HRCT was 88%, with a specificity of 74%.
CT obtained using 10-mm slice thickness is inadequate for the diagnosis of bronchiectasis, with a sensitivity of only 60% to 80% (29, 30, 31,69, 70, 71, 72). The use of HRCT or thin-slice SCT results in significant improvement in sensitivity and accuracy.
Grenier et al. (73), using 1.5-mm-thick sections obtained every 10 mm, retrospectively compared CT and bronchography in 44 lungs in 36 patients and found that CT confirmed the diagnosis of bronchiectasis with a sensitivity of 97% and a specificity of 93%. Young et al. (32) also assessed the reliability of HRCT in the assessment of bronchiectasis, as compared with bronchography, in 259 segmental bronchi from 70 lobes of 27 lungs. HRCT was positive in 87 of 89 segmental bronchi shown to have bronchiectasis (sensitivity 98%). HRCT was negative in 169 of 170 segmental bronchi without bronchiectasis at bronchography (specificity 99%). Similar results have been reported by Giron et al. (74).
It should be emphasized that, despite the excellent sensitivity of HRCT, bronchiectasis may be focal and exceedingly subtle on HRCT scans. Cylindrical bronchiectasis, in particular, can be missed on HRCT, especially if care is not taken to obtain images in deep inspiration (73, 74, 75). Giron et al. (74), in a study of 54 patients with bronchographic evidence of bronchiectasis, found that they missed three patients, all with mild cylindrical bronchiectasis, using 1-mm slices obtained every 10 mm.
The introduction of SCT has led to a reconsideration of optimal scan protocols in patients with suspected bronchiectasis. In a study by Lucidarme et al. (76) of 50 consecutive patients with suspected bronchiectasis, 1.5-mm HRCT sections obtained at 10-mm intervals were compared with a volumetric acquisition using 3-mm collimation. These authors found volumetric data acquisition to be more accurate than routine HRCT for the identification of bronchiectasis. Specifically, bronchiectasis was noted in 77 segments (22 patients) on thin-section CT scans compared with 90 segments (26 patients) on helical CT scans. Interobserver agreement was significantly better (p <.05) in identification of segments that were positive for bronchiectasis on helical CT scans (κ = 0.87) than on thin-section CT scans (κ = 0.71). Although helical CT failed to identify bronchiectasis in seven segments in which the disease was diagnosed with HRCT, in four cases a diagnosis of subsegmental cylindrical bronchiectasis was made only with helical CT. In comparison, there were no patients in whom a diagnosis of bronchiectasis was established by HRCT alone.
SCT shows greatest promise in the diagnosis of subtle cylindrical bronchiectasis. The absence of bronchial tapering is often difficult to diagnose using noncontiguous 1-mm sections.
TECHNICAL CONSIDERATIONS IN THE CT DIAGNOSIS OF BRONCHIECTASIS
Most important for accurate evaluation of bronchiectasis is the use of appropriate window level and mean, especially in those cases for which quantitative information is desired. As first shown by Webb et al. (41) using phantoms composed of Lucite cylinders, an optimal window level for assessing the airway lumen and walls is −450 HU. A similar conclusion was reached by McNamara et al. also using a reference phantom (42,77). In distinction, others have suggested that window width is as important as or more important than window level in airway measurements. Bankier et al. (78), using inflation-fixed lungs to evaluate the effect of window width and levels on bronchial wall thickness confirmed by planimetry, concluded that an optimal window width should vary between 1,000 and 1,400 HU and that window levels could vary as much as −250 to −700 HU. In our experience, for practical purposes, these windows and levels are adequate for routine visual assessment.
Standard CT protocols for the assessment of suspected airway disease and bronchiectasis have generally involved the use of HRCT obtained at spaced intervals (e.g., 10 mm) (32,73,74). Such HRCT protocols have proved highly accurate. However, the development and evolution of multidetector SCT scanners are changing our approach to the diagnosis of this disease. Using multidetector SCT, the entire thorax may be imaged volumetrically, with scans being viewed using varying slice thicknesses and in different planes after completion of the study (79,80).
SCT with a slice thickness of 3 mm or less has proved comparable to or superior to spaced HRCT images in making the diagnosis of bronchiectasis and determining its extent. It is most advantageous for the diagnosis of subtle cylindrical bronchiectasis. For example, as reviewed in the preceding section, Lucidarme et al. (76) found that a volumetric spiral acquisition using 3-mm collimation was more accurate than routine HRCT (1.5-mm HRCT sections obtained at 10-mm intervals) in the identification of bronchiectasis. Although SCT failed to identify bronchiectasis in seven segments in which the disease was diagnosed with HRCT, in four cases a diagnosis of subsegmental cylindrical bronchiectasis was made only with helical CT. In comparison, in no patients was a diagnosis of bronchiectasis established by HRCT alone.
Similarly, in a study using multidetector SCT, both 3-mm-thick and 1-mm-thick slices were reconstructed in 40 patients suspected of having bronchiectasis (4 × 1-mm detectors, 120 kV, 0.5 sec/rotation, 80 mA/slice, pitch of 1.75) (81). No significant differences were found between 3-mm-thick and 1-mm-thick slices in the detection of bronchiectasis, the evaluation of bronchiectasis extent, or the characterization of bronchiectasis type (81).
With multidetector SCT, the entire thorax may be scanned in a single breath hold using a 1- to 1.25-mm detector width. This enables reformation of the scan data in any plane, with similar spatial resolution. Viewing the scan data in multiple planes may be advantageous in the diagnosis of bronchiectasis. For example, in one study, the effectiveness of coronal reconstructions of multidetector CT (120 kVp, 70 mA, 2.5-mm collimation, table speed of 15 mm/sec, table rotation time 1 sec) (82) was assessed in the diagnosis of bronchiectasis. In 110 patients who were suspected of having bronchiectasis, both axial (2.5-mm slice thickness) and coronal (1.3- to 2.0-mm slice thickness) reformatted images were reconstructed. With axial images only, the detection rate of bronchiectasis on a per-patient basis was 97%, whereas the detection rate was 100% with both axial and coronal images (p = .0001). Also, the readers’ confidence as to the distribution of bronchiectasis was greater when both axial and coronal images were viewed (p = .008) (82). In another study (83), the use of multiplanar reconstruction of 1-mm multidetector CT resulted in improved agreement between observers as to the diagnosis of bronchiectasis (kappa improved from 0.29 to 0.54) (83).
Furthermore, the use of reconstruction techniques such as maximum-intensity projection (MIP) and minimum-intensity projection (MinIP) images and precise internal and external volumetric renderings of the airways are of potential value in the diagnosis of bronchiectasis, as is the possibility of creating CT bronchograms (84,85).
Although volumetric CT results in a greater radiation dose than does spaced HRCT scanning, low-dose volumetric CT may be used with a significant reduction in radiation but without loss of diagnostic information (86). In one study, 52 patients with suspected airway disease were studied using both spaced HRCT (120 kVp, 170 mA, 1-mm collimation, and 10-mm intervals) and low-dose volumetric SCT (120 kVp, 40-mA, 3-mm collimation, pitch of 2, and reconstruction interval of 2 mm). Eighty-six percent and 90% of patients were diagnosed with bronchiectasis at HRCT and low-dose helical CT, respectively. Of 928 segments evaluated by five observers, bronchiectasis was seen in 152.5 segments on HRCT and in 193.5 segments on helical CT. The radiation dose of the 40-mA helical technique averaged 3.21 mGy as compared with 2.17 mGy for HRCT (86). In another study (87), the image quality of multidetector CT scans (120 kVp, a 2.5-mm collimation, pitch of 6, 2.5-mm reconstruction interval) obtained in patients with suspected bronchiectasis was assessed with six different mA settings (170, 100, 70, 40, 20, 10 mA). Independently, two chest radiologists assessed and compared the quality of the images obtained at the six mA exposures. The mean image quality at exposures of 170, 100, and 70 mA were similar, and images obtained at 70 mA were rated significantly better than those obtained at 40 mA or less (p <.01). The mean radiation doses at 170, 100, 70, 40, 20, and 10 mA were 23.72, 14.39, 10.54, 5.41, 2.74, and 1.50 mGy, respectively (87).
The use of low-dose HRCT techniques for performing routine follow-up scans in patients with severe chronic disease has also been suggested (44,88). Bhalla et al. (44), evaluating scans obtained using both 70 and 20 mA showed that high-quality HRCT images of bronchiectatic airways could be obtained in patients with cystic fibrosis.
Given these options, it is apparent that choice of scan technique depends on the type of scanner available as well as available postprocessing capabilities. It is also likely that specific protocols will continue to evolve with continued clinical experience.
HRCT or multidetector SCT may also be used to evaluate the presence of air trapping in patients with suspected bronchiectasis (60,89, 90, 91, 92, 93). This may be accomplished either by repeatedly acquiring scans at one preselected level during a forced expiration or as two separate acquisitions, first in deep inspiration followed by scans obtained through the same region in expiration (18,60,79,91,94, 95, 96, 97, 98). This technique of paired inspiratory and expiratory images may be obtained using HRCT or spiral, volumetric techniques. It should be emphasized that although a variety of protocols for acquiring expiratory scans have been proposed, including volumetric expiratory imaging, 1-mm images obtained at three levels (aortic arch, tracheal carina, and above the diaphragm) are usually sufficient to identify significant air trapping, even when inspiratory scans are normal (91).
ASSESSMENT OF BRONCHIECTASIS EXTENT AND SEVERITY
Systems for grading the severity and extent of bronchiectasis by using CT findings have been proposed by various authors and have been used primarily in the assessment of patients with cystic fibrosis (CF). Bhalla et al. (44), in the first description of such a system, used nine separate variables, including the extent of mucus plugging, peribronchial thickening, generations of bronchial divisions involved, number of bullae, and the presence of emphysema, to calculate a global CT score. Based on this approach, CT was found to be a valuable tool for objectively evaluating the extent and severity of bronchiectasis in patients with CF (44).
Subsequent modifications of this system have been proposed by a number of authors (20,28,47,99, 100, 101, 102), including differences in the definition of bronchial dilatation, bronchial wall thickening, and the extent of bronchiectasis. For example, although Bhalla et al. (44) assessed segments in their scoring system, Smith et al. (20) and others have assessed bronchiectasis extent by lobes, using a five-point scale based on the visual assessment of the number of abnormal bronchi (<25%, 25% to 49%, 50% to 74%, or >75%).
Other differences among scoring systems include the methods of describing the axial extent of disease. Some investigators assess the number of generations of airways involved (44,101,102), whereas others localize abnormal airways either in the peripheral half or one third of the lung (28,47,99) or describe the overall extent of disease as assessed regionally by lobe and zone (100). More recent scoring systems have also emphasized the inclusion of centrilobular nodules and mosaic perfusion as additional signs of airway disease (47,99,101,102).
Despite these differences, most reports have shown good correlation between the HRCT assessment of bronchiectasis extent and severity when compared with more traditional radiographic, clinical, or functional criteria for assessing CF patients (20,44,47,101,102). For example, Shah et al. (47), found that HRCT severity scores in symptomatic and asymptomatic patients correlated with FVC (r = 0.44, p = .01) and FEV1 (r = 0.34, p = .04), and severity of bronchiectasis correlated with FVC (r = 0.50, p = .004) and FEV1 (r = 0.40, p = .02). In symptomatic patients, improvement in HRCT score correlated with changes in FEV1/FVC (r = 0.39, p = .049).
A relationship between the severity and extent of bronchiectasis and lung function also has been shown in patients who have other causes of airway diseases. Although largely assessing the same parameters, different investigators have tended to use slightly different criteria for determining the severity and extent of bronchiectasis and relating these findings to lung function or symptoms. Despite these differences, similar conclusions have been reached in several studies. The degree of bronchial wall thickening and the severity and extent of bronchiectasis correlate with PFT findings of obstruction (13,93,103,104) as do the extent of mosaic perfusion or air trapping (103,104). On multivariate analysis, bronchial wall thickness has proved to be the strongest independent determinant of airflow obstruction (93,103). In one study (103), the severity of symptoms tended to correlate with either bronchial wall thickening or the presence of small airway abnormalities.
For example, Lynch et al. (13) studied 261 patients with symptomatic bronchiectasis, excluding patients with CF, allergic bronchopulmonary aspergillosis, and fungal or mycobacterial infections. There was a weak but significant correlation between the degree of morphologic abnormality on CT and the extent of physiologic impairment. Scores for the severity and extent of bronchiectasis correlated with the FEV1 (r = −0.362, p = .0001) and the FVC (r = −0.362, p = .0001). Scores for bronchial wall thickening correlated with the FEV1 (r = −0.367, p = .0001) and FVC (r = −0.239, p = .001).
Similarly, in a study by Roberts et al. (93) of 100 patients with bronchiectasis, the extent and severity of bronchiectasis and the severity of bronchial wall thickening correlated strongly with the severity of airflow obstruction; the closest relationship found was between decreased FEV1 and the extent of decreased attenuation on the expiratory scan (r = −0.55, p <.00005). On multivariate analysis bronchial wall thickness and decreased attenuation were the strongest independent determinants of airflow obstruction. The severity of bronchial dilatation was negatively associated with airflow obstruction.
In another study, the severity of bronchial wall thickening and the extent of bronchiectasis, small airway abnormalities (i.e., centrilobular nodules, tree-in-bud, and bronchiolectasis), and mosaic perfusion were evaluated in 60 patients with bronchiectasis and associated with clinical and functional parameters (103). The frequency of clinical exacerbations was associated with the degree of bronchial wall thickening (r = 0.29, p = .04) and the 24-hour sputum volume correlated with bronchial wall thickening and small airway abnormalities (r = 0.30, p = .03 and r = 0.39, p = .004, respectively). The extent of bronchiectasis, bronchial wall thickening, and mosaic perfusion, respectively, were related to FEV1 (r = −0.43 to −0.60, p <.001), forced expiratory flow, midexpiratory phase (FEF25%-75%) (r = −0.38 to −0.57, p <.001), FVC (r = −0.36 to −0.46, p <.01), and FEV1/FVC ratio (r = −0.31 to −0.49, p <.01). After multiple regression analyses, bronchial wall thickening remained a significant determinant of airflow obstruction, whereas small airway abnormalities remained associated with 24-hour sputum volume (103).
Only gold members can continue reading. Log In or Register to continue