the center of the secondary pulmonary lobule. Between these core structures and the interlobular septa, numerous alveolar spaces, capillaries, and respiratory bronchioles are present. This accounts for the characteristic centrilobular distribution of bronchiolar abnormalities detected on thin-section CT scans (7, 8, 9).
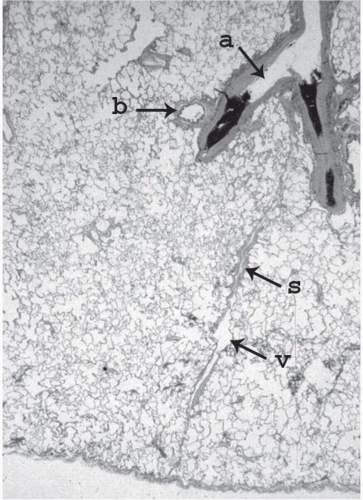 Figure 5-1 Histologic appearance of a secondary pulmonary lobule. The lobular bronchiole (b) is accompanied by its homologous pulmonary artery filled with a clot (a). The interlobular septum (s) contains the interlobular vein (v). |
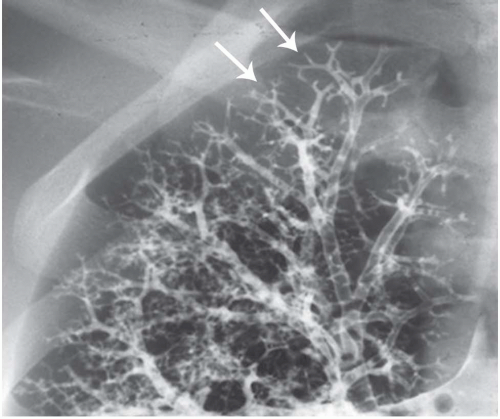 Figure 5-2 Normal bronchogram of the right bronchial tree targeted on the right upper lobe. The arrows show the normal appearance of lobular and terminal bronchioles. |
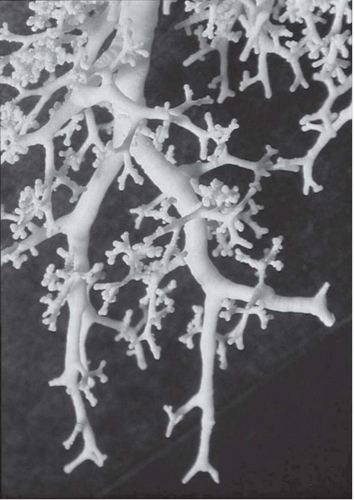 Figure 5-3 Bronchial cast from a human lung specimen showing the origin and divisions of several terminal bronchioles. (Courtesy of Ewald Weibel.) |
correlation with the clinical and radiologic manifestations of disease. The histologic classification also shows better correlation with the natural history of the disease and its response to therapy.
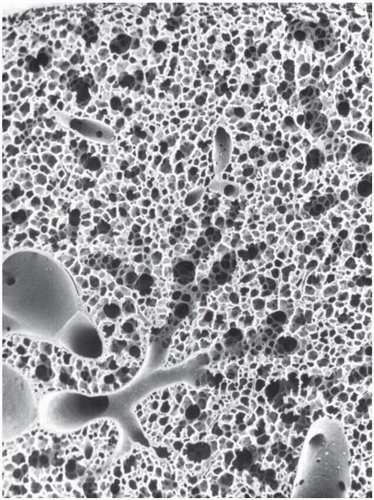 Figure 5-4 Low-power scanning electron microscopy of a normal lung specimen showing the origin and the divisions of terminal and respiratory bronchioles down to the alveolar ducts and sacs. (Courtesy of Ewald Weibel.) |
TABLE 5-1 ETIOLOGIES AND CLINICAL CONDITIONS ASSOCIATED WITH BRONCHIOLITIS | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
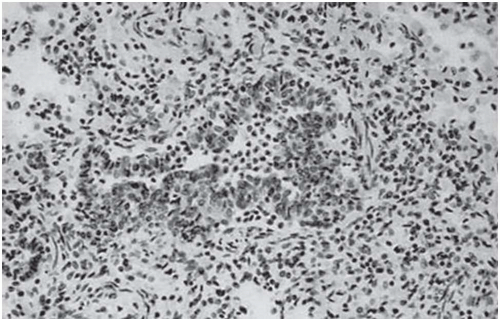 Figure 5-5 Cellular bronchiolitis. Surgical biopsy (×20) with immunohistochemical labeling. Inflammatory bronchiolitis caused by respiratory syncytial virus infection. |
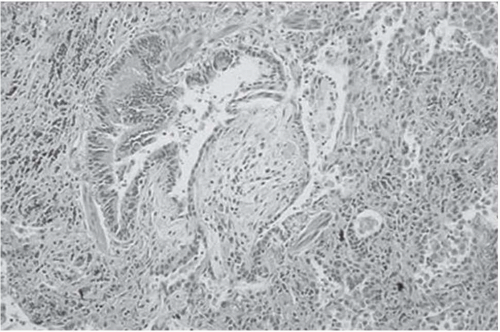 Figure 5-6 Bronchiolitis obliterans with intraluminal polyps. Surgical biopsy (×20, hematoxylin and eosin) obliteration of the lumen of a respiratory bronchiole by a fibroblastic plug floating in the lumen. The same type of fibroblastic reaction is also present in more distal airspaces (organizing pneumonia). |
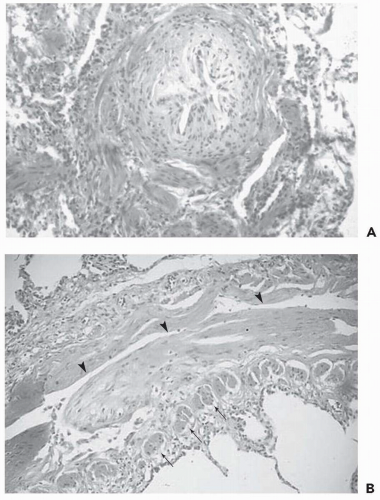 Figure 5-7 Obliterative (constrictive) bronchiolitis. Surgical biopsy (×20, HE). A: Section perpendicular to a terminal bronchiole showing a concentric narrowing of the bronchiolar lumen by subepithelial fibrosis. B: Section along the long axis of another terminal bronchiole showing the longitudinal extent of the subepithelial fibrosis. Arrows show the section of the smooth muscle fibers in the bronchiolar wall. Arrowheads show the narrowed bronchiolar lumen. |
TABLE 5-2 CONDITIONS ASSOCIATED WITH OBLITERATIVE BRONCHIOLITIS | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||
centrilobular nodule a few millimeters in diameter. In every case, the key feature is the centrilobular location of these opacities, at least 3 mm from the pleura.
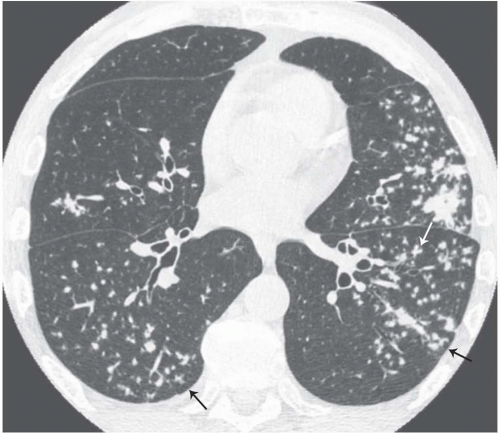 Figure 5-8 Tree-in-bud sign. Endobronchial spread of tuberculosis. Bilateral patchy areas of small centrilobular, nodular, and/or linear branching opacities. Note also the presence of larger nodules and an airspace consolidation in the left upper lobe. |
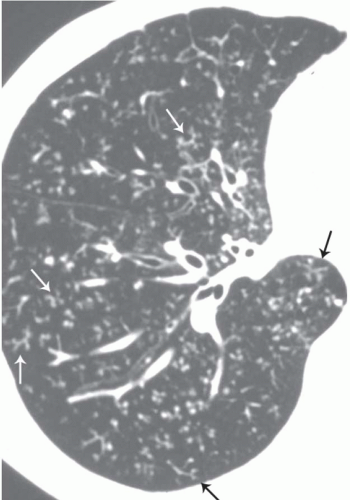 Figure 5-9 Tree-in-bud sign. Thin-section CT targeted on the right lung in a patient with diffuse aspiration bronchiolitis secondary to esophagobronchial fistula seen as a complication of cancer of esophagus. There are multiple small centrilobular nodular and/or branching linear opacities. Some arrows show typical tree-in-bud sign. |
 Figure 5-10 Tree-in-bud sign. A 5-mm-thick coronal slab using the multiplanar volume reformation combined with maximum intensity projection technique after thin-collimation multidetector CT acquisition. Multiple areas of small centrilobular, nodular, and/or linear branching opacity become apparent in the posterior segment of the right upper lobe (arrow). This helped the endoscopist perform a selective bronchial aspiration, which permitted the diagnosis of tuberculosis. |
vasculitis, pulmonary hypertension, sarcoidosis, or, rarely, BOOP. When the distribution of nodules is diffuse and homogeneous, the pattern is suggestive of bronchiolar disease or vascular entities, including pulmonary edema, pulmonary hemorrhage, and capillary hemangiomatosis. Differential diagnosis with bronchiolar disease is based on associated findings, such as pleural effusion in edema and enlargement of proximal pulmonary arteries. Bronchiolar possibilities include respiratory bronchiolitis, bronchiolitis associated with hypersensitivity pneumonitis, and follicular bronchiolitis (7,40). Despite the large number of diseases potentially responsible for this pattern, in most cases the differential diagnosis is simplified by detailed clinical information, including occupational and environmental histories.
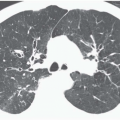
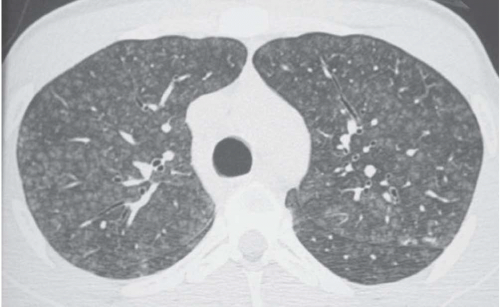 Figure 5-11 Poorly defined centrilobular nodules. Subacute hypersensitivity pneumonitis (bird fancier’s lung). Thin-section CT scan shows diffuse and homogeneous distribution throughout the lungs of the small centrilobular opacities expressing the inflammation in the bronchial and peribronchial areas. |
attenuation, more or less associated with poorly defined centrilobular nodular opacities, is a CT pattern frequently observed in acute or subacute hypersensitivity pneumonitis (Fig. 5-14) (49).
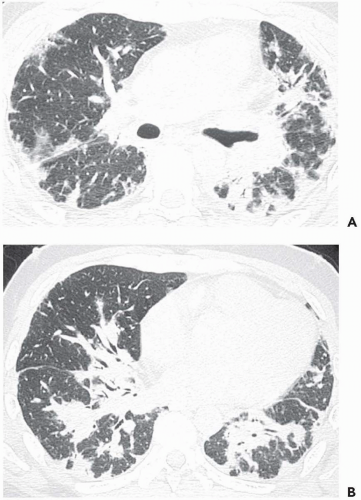 Figure 5-12 Airspace consolidation. Cryptogenic organizing pneumonia. Bilateral areas of airspace consolidation having both peripheral and peribronchovascular predominant distribution. A: Thin-section CT at the level of upper lobes and superior segments of lower lobes. B: Thin-section CT scan at the level of lower lobes. |
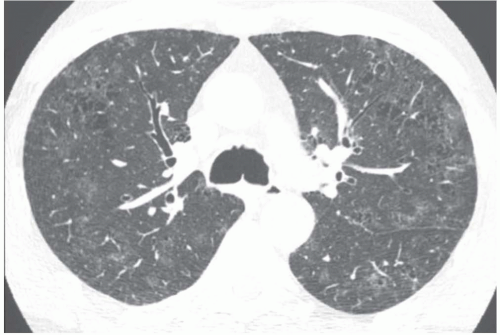 Figure 5-13 Ground-glass opacity. RB-ILD. Thin-section CT at the level of the main bronchi in a heavy smoker suffering from chronic dyspnea and cough. Patchy areas of ground-glass attenuation are present within the peripheral part of the lungs. Multiple spaces of centrilobular emphysema and bronchial wall thickening are also present. The abnormalities are related to RB-ILD. |
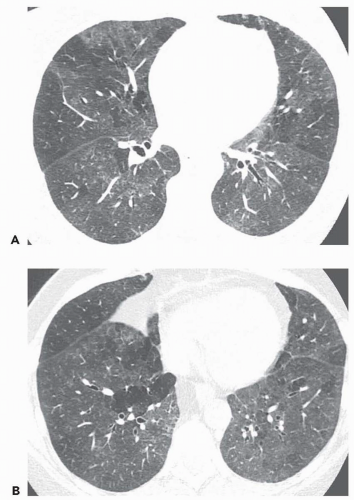 Figure 5-14 Ground-glass opacity and mosaic attenuation pattern. Subacute hypersensitivity pneumonitis (bird fancier’s lung). A and B: Two thin-section CT scans through the mid (A) and lower (B) parts of the lung. Multiple patchy areas of ground-glass attenuation are associated with small, poorly defined centrilobular nodules. Notice also the presence of some secondary pulmonary nodules appearing hypoattenuated and free of nodules, reflecting the presence of air trapping. |
(55,56) and, less often, primary pulmonary hypertension (57), pulmonary capillary hemangiomatosis (58), pulmonary venoocclusive disease (59), polyarteritis nodosa (52), scleroderma (57), and intimal sarcoma of the pulmonary arteries (60). The differential diagnosis between a bronchiolar and a vascular cause can be based on the presence or absence of air trapping on expiratory CT, respectively (54,61). When caused by bronchiolar obstruction, mosaic perfusion is accentuated on expiratory CT because the low-attenuation areas show air trapping (Fig. 5-17). In chronic vascular occlusive disease, air trapping theoretically does not occur. However, in a study by Worthy et al. (52) applying the previously mentioned criteria to distinguish diseases that may cause mosaic pattern of lung attenuation on CT scans, two observers made a correct diagnosis in 90% of infiltrative lung disease cases, 91% of airway disease, and only 32% of vascular disease. The difficulty in the diagnosis of vascular disease was the result of the presence of expiratory air trapping in a certain number of cases (52). This phenomenon was
confirmed recently by Arakawa et al. (62), who found expiratory air trapping in six of nine patients with chronic embolism. Air trapping was associated with the presence of proximal arterial stenosis (p <.01), and the area showed less contrast enhancement than did the adjacent lung (p <.05).
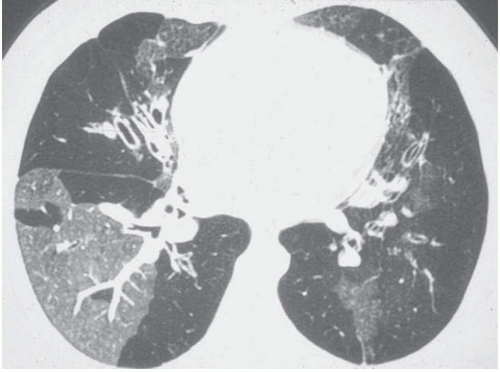 Figure 5-15 Mosaic perfusion pattern. Postinfectious obliterative bronchiolitis. Thin-section CT scan in a 14-year-old boy suffering from shortness of breath at exercise. The hyperattenuated area contains enlarged vessels, reflecting the pulmonary blood flow distribution toward the normal ventilated areas. Hypoattenuated areas are extended in both lungs and contain few and small pulmonary vessels. Bronchiectasis is also present in the right middle lobe and the left lower lobe. The demarcation between normal and abnormal areas is well defined, reflecting the limits between segments and lobules. (Courtesy of Christopher Flower.) |
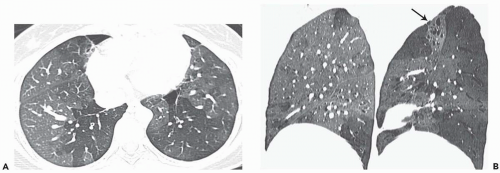 Figure 5-16 Mosaic perfusion pattern at MDCT. Postinfectious bronchiolitis. Thin-collimation MDCT acquisition. A: Thin-section CT at the level of the lower part of the lungs showing patchy areas of hypoattenuation in the lower lobes and the right middle lobe. B: Lateral reformation after thin-collimation multidetector row CT acquisition using the multiplanar volume reformation and minimum-intensity projection techniques in combination. Left (sagittal reformation of the right lung) and right (sagittal reformation of the left lung) images show well-demarcated areas of hypoattenuation and decreased perfusion, reflecting the territories where the lesions of obliterative bronchiolitis are situated. Notice the presence of bronchiectasis in the apicoposterior segment of the left upper lobe (arrow). |
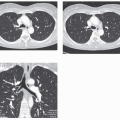
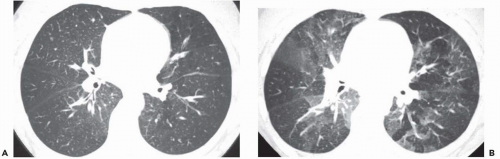 Figure 5-17 Mosaic perfusion and expiratory air trapping. Postinfectious obliterative bronchiolitis. Thin-section CT scan performed at full inspiration (A) and full expiration (B) of the middle parts of the lungs. On inspiratory scan, mosaic perfusion pattern is difficult to perceive. There is only mild hypoattenuation in the periphery of the left lung and the peripheral part of the right upper and lower lobes. At expiration, the contrast in attenuation between normal and abnormal areas is accentuated. The normally ventilated areas increase in attenuation at expiration as normally expected, whereas the abnormal areas do not, because of air trapping. |
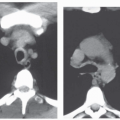
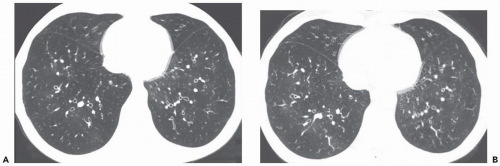 Figure 5-18 Decreased lung attenuation and expiratory air trapping. Thin-section CT scans obtained at full inspiration (A) and full expiration (B) in a patient presenting with post-bone marrow transplantation obliterative bronchiolitis. A: On inspiratory scan, there is a diffuse decrease in attenuation throughout the lungs with a paucity of pulmonary vessels in the periphery, expressing a severe and diffuse distribution of the bronchiolar obstructive lesions. Notice also the presence of bronchial wall thickening and slight dilatation of the bronchial lumen within the lower lobes. B: On expiratory scans, there is no significant increase in attenuation of the lung parenchyma. The cross-sectional areas of the lungs are not very different from those at inspiration, expressing the presence of bilateral and diffuse expiratory air trapping. |
phenomenon reflects the presence of air trapping in areas where partial airway obstruction is present (69, 70, 71, 72). These areas are commonly well demarcated, reflecting the geometry of individual or joined lobules. This pattern is frequently observed in smokers and in patients with asthma (Fig. 5-20), obliterative bronchiolitis, bronchiolitis associated with hypersensitivity pneumonitis (Fig. 5-21), or sarcoidosis (Fig. 5-19). In addition, this pattern may also be seen in patients with acute pulmonary embolism (73). Arakawa et al. (73) found in a series of 41 patients with acute pulmonary embolism one or more areas of air trapping in 72% of the patients. This air trapping was seen not only in areas with pulmonary embolism but also in areas without embolism. The proposed mechanism of bronchoconstriction in acute pulmonary embolism includes bronchoactive amines released from platelet aggregations in the thrombus or a change in parasympathetic nervous system tension, which centralizes the bronchial smooth muscle tension.
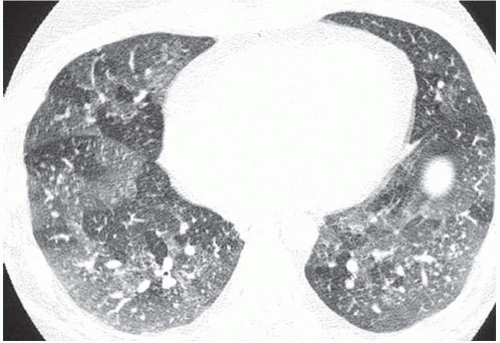 Figure 5-19 Lobular areas of expiratory air trapping. Early stage of sarcoidosis. Thin-section CT obtained at full expiration. Several lobular areas in both lungs did not increase in attenuation as normally expected. There was no abnormality depictable on inspiratory scans performed at the same anatomic level. |
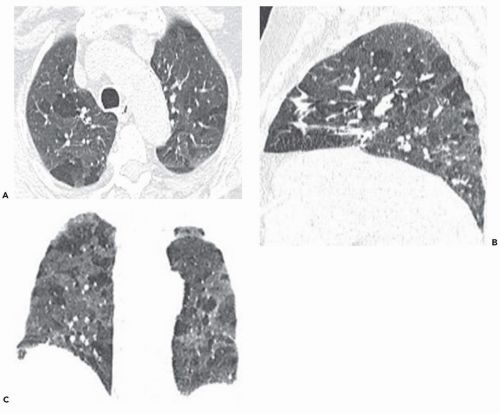 Figure 5-20 Lobular areas of air trapping at MDCT. Mild persistent asthma. Low-dose thin-collimation MDCT acquisition performed at maximum expiration. A: Axial thin-section CT shows lobular areas of air trapping in the upper lobe. B: Sagittal reformation of the right lung displays the upper and posterior distribution of lobular areas of air trapping. C: Coronal reformation with minimal intensity projection technique displays the extent of air trapping in both lungs. |
gradient can have a lobar component on expiratory scan; the posterior aspect of the upper lobe, anterior to the major fissure, often appears denser than the anterior aspect of the lower lobe, behind the major fissure. Some focal areas of low attenuation may also be seen near the tip of the lingula. All these physiologic low-attenuation areas involve less than 25% of the cross-sectional area of one lung at one scan level. As a result, air trapping can be considered abnormal when it affects nondependent areas or dependent lung areas greater than 25% of the lung cross-sectional area or a lung volume equal to or greater than a pulmonary segment and is not limited to the superior segment of the lower lobe.
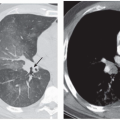
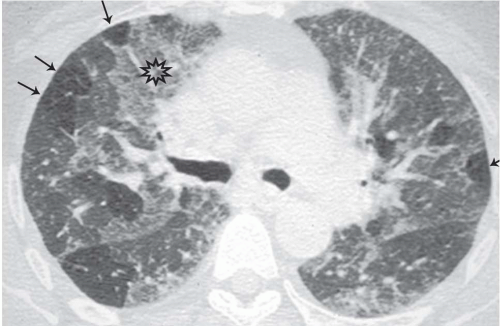 Figure 5-21 Ground-glass, mosaic perfusion, and lobular areas of air trapping (“head cheese” pattern). Subacute hypersensitivity pneumonitis. Expiratory thin-section CT at the level of the upper part of the lungs, showing patchy areas of ground-glass attenuation (star), combined with normal areas and some lobules appearing hypoattenuated because of air trapping (arrows). |
emphysema, panlobular emphysema, constrictive bronchiolitis, and normal lung on the basis of texture features. The proposed technique discriminates well among patterns of obstructive lung disease on the basis of parenchymal texture alone, with good sensitivity and good specificity (Fig. 5-24).
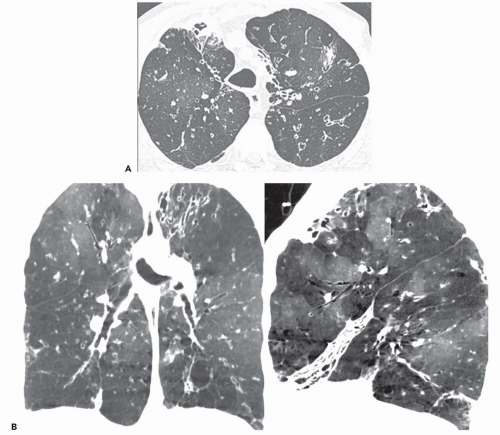 Figure 5-22 Minimum-intensity projection and mosaic perfusion pattern. Postinfectious bronchiectasis and obliterative bronchiolitis. A: Thin-section axial CT scan at the level of the upper part of the lungs. Distortion and enlargement of the lumen of the trachea with bilateral cylindrical bronchiectasis in the upper lobes and the superior segment of the left lower lobe. Slight heterogeneity in lung attenuation. B: Multiplanar volume reformation combined with minimum intensity projection technique after thin-collimation MDCT acquisition. The coronal (left) and sagittal (right) reformations reinforce the detection of mosaic perfusion pattern and help assess the extent of decreased attenuation areas in both lungs. Notice the presence of a nonaerated collapse of the right middle lobe associated with bronchiectasis (right). |
patients with good results despite a longer scanning time per image (83,84). Motion artifacts, which increase as temporal resolution decreases, represent the major limitations of continuous expiratory CT. The use of 180-degree linear interpolation algorithms with a 0.5-second rotation time provides images representing scanning periods of about 250 msecond. Motion artifacts are at maximum during the early phase of expiration and at a minimum during its late phase, which allows good visualization of lobular air trapping with helical CT.
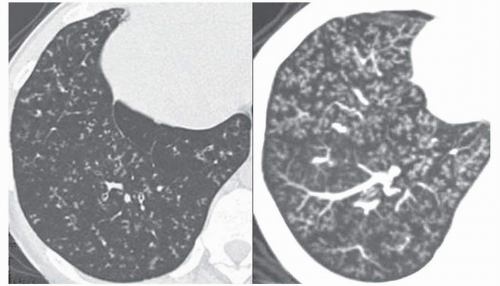 Figure 5-23 Tree-in-bud sign. Infectious bronchiolitis in a patient with ciliary dyskinesia. Left: Thin-section CT targeted on the right lower lobe showing multiple small centrilobular, nodular and linear branching opacities in many lobules of the right lower lobe. Right: A 7-mm-thick axial slab using the multiplanar volume reformation and maximum-intensity projection technique, increasing the profusion of the small centrilobular opacities and keeping the same spatial resolution of thin-section CT scan in infectious bronchiolitis. |
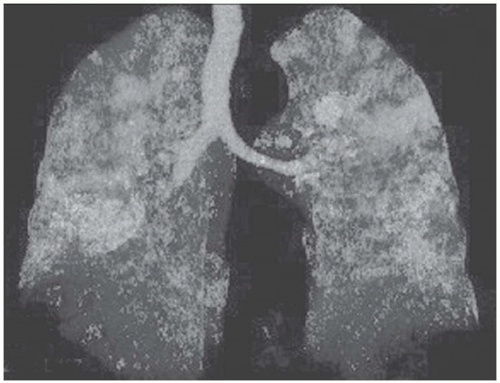 Figure 5-24 Three-dimensional (3D) display of expiratory air trapping. Same patient as in Figure 5-20. The areas of hypoattenuation resulting from expiratory air trapping are automatically segmented and highlighted and taken into account in the 3D reconstruction.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|