Bronchocentric Granulomatosis
Jud W. Gurney, MD, FACR
Key Facts
Terminology
Pathologic reaction characterized by bronchocentric necrotizing granulomatous process in which airway wall is replaced by granulomatous tissue and palisaded histiocytes
Airway lumen usually filled with necrotic debris
Multiple causes, divided into infectious and noninfectious (usually allergic)
Imaging Findings
HRCT: Peripheral bronchiectasis or mucus plugging
Nodule or mass lesions (60%)
Size 2-6 cm, unilateral (60%), solitary (75%) (when multiple usually < 3 in number)
Upper lobe location (60%)
Consolidation (30%)
Lobar (25%); for those not lobar, usually consolidation greater than segment in size
Diffuse reticulonodular pattern (10%)
Top Differential Diagnoses
Bronchogenic Carcinoma
Allergic Bronchopulmonary Aspergillosis
Wegener Granulomatosis
Pathology
Necrotizing granulomatous reaction centered around airways hallmark
Clinical Issues
Asthma (50%), tissue eosinophilia, fungal (Aspergillus) hyphae on biopsy, similar to ABPA
Nonasthmatic(50%), have neutrophils in lung lesions, no asthma, no microscopic evidence of fungi
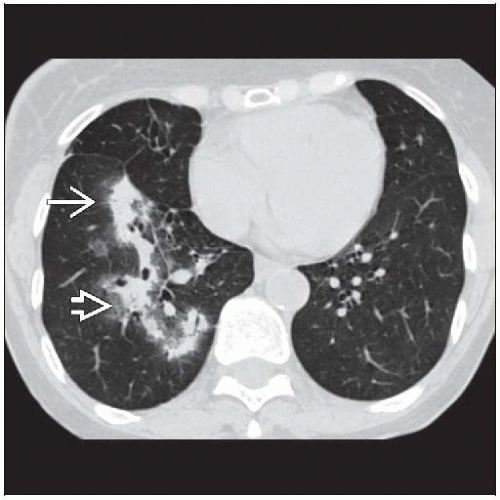 Axial HRCT shows nodular consolidation clustered along the airways  . A larger area of consolidation has a spiculated margin . A larger area of consolidation has a spiculated margin  . . |
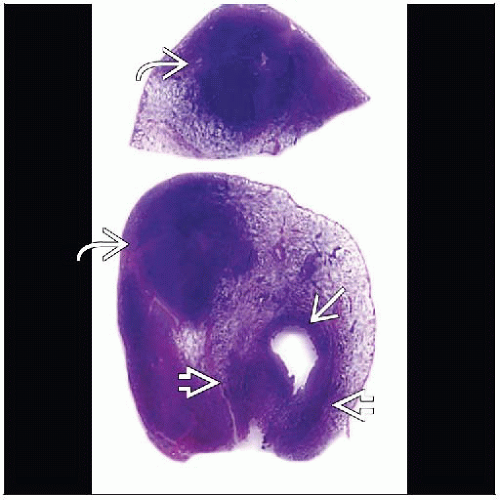 Macroscopic pathology slide shows dilated bronchus  surrounded by inflammatory tissue surrounded by inflammatory tissue  . The bronchus is also obliterated by inflammatory tissue . The bronchus is also obliterated by inflammatory tissue  . . |
TERMINOLOGY
Abbreviations and Synonyms
Bronchocentric granulomatosis (BCG), allergic bronchopulmonary aspergillosis (ABPA)
Definitions
Pathologic reaction characterized by bronchocentric necrotizing granulomatous process in which airway wall is replaced by granulomatous tissue and palisaded histiocytes
Airway lumen usually filled with necrotic debris
Multiple causes, divided into infectious and noninfectious (usually allergic)
IMAGING FINDINGS
General Features
Best diagnostic clue: Focal air-space mass or peripheral bronchiectasis and mucoid impaction
Patient position/location: Slightly favors upper lobes
Size: Air-space mass usually several cm in size
Morphology: Mass usually has spiculated margin
CT Findings
Nonspecific, 3 patterns
Radiographic patterns same no matter which clinical presentation
Air-space findings
Nodule or mass characteristics
Spiculated margin, 2-6 cm in size
Location: Upper lobes or superior segments of lower lobes
CT more sensitive for cavitation (air or fluid)
Contain air-bronchograms signifying air-space process
Consolidation
Lobar with mild volume loss
Mucoid impaction
May have multilobar disease (contralateral upper lobe)
Central airways patent (if central obstruction, consider bronchogenic carcinoma, which may have a pathologic pattern of BCG in the postobstructive lung)
Airways findings
Other
Mediastinal lymph node enlargement (< 10 mm short axis diameter) common
Pleural effusions uncommon
Radiographic Findings
Radiography
Nodule or mass lesions (60%)
Size 2-6 cm
Unilateral (60%), bilateral (40%)
Solitary (75%), when multiple usually < 3 in numberRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



